|
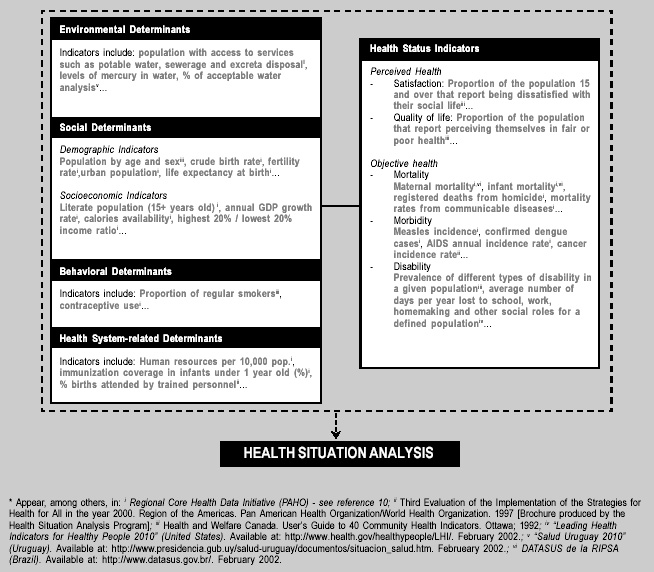
Figure 1: Examples of Indicators of the Health Status
and some of its Determinants*
|
 |
-from Epidemiological Bulletin, Vol. 22 No. 4, December 2001-
The availability of information based on valid, reliable data is a sine qua non condition for the analysis and objective evaluation of the health situation, evidence-based decision-making and programming in health. The search for objective measures of a population’s state of health is an old tradition in public health, particularly in epidemiology. Starting with the works of William Farr in the 19th century, health descriptions and analyses were, for a long time, based on measures of mortality and survival.(1,2) The need for considering other dimensions of a population’s health status was recognized more recently. This realization came in part as a result of the successful control - mostly in the most industrialized areas - of infectious diseases that were traditionally responsible for the greatest burden of mortality. It is also the product of a more comprehensive vision of health and its population determinants. As a consequence, measures of morbidity, disability and non-biological determinants of health (such as access to services, quality of care, living conditions and environmental factors) are increasingly necessary to document people’s capacity to function physically, emotionally and socially, as well as to objectively analyze the health situation (See figure 1).(3) Health indicators facilitate the quantification and evaluation of these different dimensions of a population’s health.
|
Figure 1: Examples of Indicators of the Health Status
and some of its Determinants*
|
|
|
A health indicator is “a construct of public health surveillance that defines a measure of health (i.e., the occurrence of a disease or other health-related event) or a factor associated with health (i.e., health status or other risk factor) among a specified population.”(4) In general terms, health indicators represent summary measures that capture relevant information on different health attributes and dimensions, and the performance of the health system. Seen together, these measures attempt to reflect and monitor the health status of a population.
The construction of an indicator is a process with various degrees of complexity, ranging from a direct count (for example of the number of new cases of malaria in a week) to the calculation of proportions, rates, ratios, and more sophisticated indices (for example life expectancy at birth).(5) Accordingly, the quality of an indicator strongly depends on the quality of its components (frequency of cases, size of populations at risk etc.) The quality of the data information, recollection, and registration systems is equally important. More specifically, the quality and usefulness of an indicator are defined by its validity (effectively measures what it attempts to measure) and reliability (repeated measurements in similar conditions produce the same results). Additional attributes to ensure quality are its specificity (measures only the phenomena that it is meant to measure), sensitivity (has the capacity to measure changes in the phenomena that it is meant to measure), measurability (is based on available or easy to obtain data), policy-relevance (is capable of providing clear responses to key policy issues) and cost-effectiveness (results justify the investment in time and other resources).(6-8) Indicators must also be easy to use and interpret by analysts, as well as understandable by information users, such as managers and decision-makers.
Important attributes to insure quality of the set of indicators are: integrity (no missing data) and internal consistency (when seen alone or in a group, the values of the indicators are realistic and coherent and do not contradict themselves).9 Therefore, the systematic use of standardized operational definitions and measurement and calculation procedures is fundamental to guarantee the quality and comparability of the indicators.(2,9)
An appropriately defined and maintained set of health indicators provides information for the elaboration of a relevant profile of a population’s health situation. The selection of such an indicators set -and its levels of disaggregation- can vary with the availability of information systems, data sources, resources, and specific needs and priorities of each region or country.2 Maintenance of an indicators set also depends on the availability of data sources and regular operation of information systems. Additionally important is the simplicity of the instruments and methods used in compiling the indicators.(9) Quality must be monitored regularly because it is crucial in building and maintaining the information users’confidence in the indicators. It is a condition for their regular use, which also depends on the indicators’ dissemination policy, including their frequency of compilation and timeliness. For example, the time lag between data collection, analysis and dissemination of an indicator used in monitoring must be short for it to maintain its relevance.(8)
When generated and administered within a functional information system, health indicators constitute a fundamental tool for decision-makers at all management levels. In general, a basic set of health indicators -such as the one that is part of the Regional PAHO Initiative of Core Health Data and Country Profiles(10) (see box)- generates evidence on the status and trends of the health situation in the population. This includes documentation of inequalities in health, which may -in turn-serve as empirical basis for the determination of population groups with the greatest health needs, stratification of epidemiological risk, and identification of critical areas. The availability of an indicators set provides the material for this analysis. Concomitantly, health indicators facilitate monitoring of health objectives and goals, strengthen the analytical capacities of health teams, and serve as a platform to promote the development of interconnected health information systems. In short, valid and reliable health indicators are basic and important epidemiological tools for health management.
|
The "Core Health Data" Initiative
|
|
The Core Health Data (CHD) Initiative was launched in 1995 to monitor the level of advancement of the health objectives and mandates adopted by PAHO/WHO and its Member States in the region of the Americas. The CHD Initiative seeks to provide a standardized information platform on the regional health situation and trends. This information can be used by managers and policy makers for: i) formulation, adjustment, and evaluation of health policies and programs; ii) reorientation of health services and public health surveillance systems; iii) programming, monitoring, evaluation, and adaptation of technical cooperation; iv) mobilization of resources; and, v) dissemination of technical health information.10 Therefore, the CHD Initiative is a process that promotes the use of epidemiology for health management, strengthening analytical capacities and creating evidence for decision-making in public health policy, including detection of health inequalities and identifying priorities for technical cooperation. CHD is part of the response by the Epidemiology Services and PAHO towards the current demand to rethink essential public health functions, increase institutions’ transparency and technical credibility, and efficiently prioritize cooperation in health.
The CHD Initiative’s principal component is its database. Including the 48 countries and territories of the Americas, the database is made up of 109 indicators disaggregated into 405 core data and their historical series since 1990. The CHD Initiative includes mortality, morbidity and access, resources and health services system coverage, socioeconomic health determinants, and environmental and demographic indicators. The Initiative includes a Web-based system allowing the user to generate tables and permitting fast access and versatile queries to the regional database. Published annually since 1995, the brochure “Health Situation in the Americas: Basic Indicators” displays 58 indicators aggregated by country and 38 aggregated by subregion. Among the CHD Initiative’s components is an up-to-date series of Country Profiles and a set of technical reference documents, including a glossary of harmonized definitions of indicators and standardized criteria for validation and data consistency. The CHD Initiative has been broadly supported by the countries of the Americas. Presently, 23 of the 35 Member States have adapted the CHD and produced national pamphlets of Basic Indicators, disaggregated at subnational levels. For example, in Argentina, Brazil, and Cuba pamphlets have been published annually since 1996 and in Costa Rica, Ecuador, Guatemala, Mexico, Nicaragua, Peru, Uruguay, and Venezuela, from 1997-98. Some countries have even attempted to extend and adapt the CHD Initiative to the local-level. Cuba maintains a disaggregated database at the municipal level; in Colombia, the department of Santander already published its departmental version and Amazonas is in the process of doing the same; Nicaragua recently published the complete set of basic indicator brochures for each of the 17 Local Integral Health Care Systems (“Sistemas Locales de Atención Integral de la Salud (SILAIS)”), which are the geographic and administrative organizational units for the health sector. In 2001, Haiti launched its first publication of the Basic Indicators. This was an impressive endeavor given the challenges presented by the structural and organizational management of health information in the country. Publication of subnational core data for Bolivia and Jamaica is imminent in 2002. Also on the agenda for 2002 is the strengthening of the Core Data Initiative in Central America within the framework of current subregional integration agreements. Experiences within countries in implementing the CHD Initiative have demonstrated the crucial importance of intersectoral coordination to guarantee the data quality and analytical use of the information. The most successful example of this type of coordination is Brazil’s Interagency Network of Information for Health (“Red Interagencial de Información para la Salud (RIPSA)”). A network of institutions, RIPSA coordinates national entities responsible for production and/or data analysis in health. Through the work of subcommittees, RIPSA is responsible for technical quality, coverage, validation, and harmonization of core data including aspects of dissemination of information. This includes maintenance of the unified health system (DATASUS) Web page, managerial use of the situation analyses, including the establishment of health situation rooms and the continuity and sustainability of the network. The CHD Initiative has formed a rich venue of technical cooperation for strengthening information systems and networks for communicating in health. CHD contributes to the creation of epidemiological intelligence for public health management and the formulation of more efficient, effective, and equitable health policies in the Americas. |
References:
(1) Hansluwka H. Measuring the health of populations, indicators and interpretations.
Soc Sci Med. 1982;20(12):1207-1224.
(2) Catford J. Positive health indicators - towards a new information base for
health promotion. Community Medicine 1983;5:125-132.
(3) Pascal J, Lombrail P. Mesure de L’Etat de Santé de la Population. La Revue
du Praticien 2001;51:1931-1938.
(4) Lengerich EJ (ed.). Indicators for Chronic Disease Surveillance: Consensus
of CSTE, ASTCDPD, and CDC. Atlanta, GA: Council of States and Territorial Epidemiologists,
November 1999.
(5) Merchán-Hamann E, Tauil PL, Pacini Costa M. Terminología das Medidas e Indicadores
em Epidemiologia: Subsídios para uma Possível Padronizaçăo da Nomenclatura.
Informe Epidemiológico do SUS 2000;9(4):273-284.
(6) Ware J, Brook R, Davies A, Lohr K. Choosing Measures of Health Status for
Individuals in General Populations. AJPH 1981;71(6): 620-625.
(7) Last J. A Dictionary of Epidemiology, Fourth Edition. New York, NY: Oxford
University Press; 2001.
(8) United Nations. A Critical Review of the Development of Indicators in the
Context of Conference Follow-up. Report of the Secretary General. Geneva:UN
Economic and Social Council; 5-30 July 1999. Document E/1999/11.
(9) Pan American Health Organization. Special Program for Health Analysis. Regional
Initiative of Core Health Data and Country Profiles 2000. Working Document.
Washington, DC; 2000. (Unedited Document).
(10) Pan American Health Organization. Collection and Use of Core Health Data.
Washington, DC:PAHO; 25 September 1997. Document CD40.R10.
Source: Prepared by the Analysis Group from PAHO's Special Program for Health Analysis (SHA).
Return to Index
Epidemiological
Bulletin, Vol. 22 No. 4, December 2001
