- Español
- English
HIV prevention in the SPOTLIGHT
An analysis from the perspective of the health sector in Latin America and the Caribbean
2017



HIV Prevention in the Spotlight: An Analysis from the Perspective of the Health Sector in Latin America and the Caribbean, 2017
ISBN: 978-92-75-11979-2
© 2017 Pan American Health Organization and Joint United Nations Programme on HIV/AIDS
All rights reserved. Publication is available on the PAHO website (www.paho.org) and on the UNAIDS website (http://onusidalac.org/1). Requests for permission to reproduce or translate this publication should be addressed to PAHO Publications through the PAHO website (www.paho.org/permissions).
Suggested citation. Pan American Health Organization and Joint United Nations Programme on HIV/AIDS. HIV Prevention in the Spotlight: An Analysis from the Perspective of the Health Sector in Latin America and the Caribbean, 2017. Washington, D.C.: PAHO, UNAIDS; 2017.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Pan American Health Organization and/or the Joint United Nations Programme on HIV/AIDS concerning the status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the Pan American Health Organization and/or the Joint United Nations Programme on HIV/AIDS in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the Pan American Health Organization and the Joint United Nations Programme on HIV/AIDS to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the Pan American Health Organization and/or the Joint United Nations Programme on HIV/AIDS be liable for damages arising from its use.
In any reproduction of this Work there should not be any suggestion that PAHO and/or UNAIDS endorse any specific organization, service, or product.
The countries of Latin America and the Caribbean have committed to ending AIDS by 2030, a clear and at the same time ambitious objective that sets the path to follow in this Region. Ending this epidemic requires special emphasis on HIV prevention, and it is in that context that the Pan American Health Organization is presenting HIV prevention in the spotlight: An analysis from the perspective of the health sector in Latin America and the Caribbean 2017, prepared in close collaboration with UNAIDS, with important contributions from civil society.
This report presents the countries’ achievements and challenges in HIV prevention and calls on them to renew their commitment and efforts to reduce new HIV infections. It also highlights the progress made toward meeting the targets set by the governments of this Region to end AIDS in the coming years. This edition is particularly timely and relevant, as the number of new HIV cases in Latin America and the Caribbean has remained constant since 2010. We have not seen the decline needed to end the epidemic.
This new edition continues the successful series of in-depth analyses of HIV in Latin America and the Caribbean that began in 2012 with Antiretroviral treatment in the spotlight. It addresses different aspects of the HIV response from a public health perspective and provides information to guide governments and partners in the improvement of their efforts.
This edition is also presented in support of the Plan of action for the prevention and control of HIV and sexually transmitted infections 2016-2021, adopted by the PAHO Member States at the 55th Directing Council of 2016.
The framework for this report is the new “combination HIV prevention” approach, which covers biomedical interventions and the promotion of healthy behaviors, as well as aspects of the enabling environments needed for the implementation of prevention measures.
The analysis and recommendations in this report focus primarily on the health sector and, in particular, the three populations most affected by the HIV epidemic: female sex workers, transgender women, and gay men and other men who have sex with men.

This publication is based on data reported by national programs throughout the Region and information furnished by civil society in more than 12 countries. Various aspects of the health sector response in HIV prevention were examined—such as access by the key populations to HIV testing, antiretroviral treatment, pre- and post-exposure prophylaxis, condoms and lubricants, and barriers to access such as discrimination in health services—in order to evaluate the progress made toward meeting the regional prevention targets.
Furthermore, this report addresses sustainability and warns about the Region’s dependence on international funds to advance prevention activities for the key populations and the challenges that this entails. The report also underscores the critical role of civil society in guaranteeing a more effective HIV response, particularly in the area of prevention.
We trust that the information presented in this publication will help all of us, as stakeholders, in our enhanced and coordinated efforts to reduce new HIV infections and end AIDS by 2030.
Dr. Carissa F. Etienne, Director
Pan American Health Organization
The world has witnessed decisive changes regarding the status of HIV over the past decade. AIDS-related deaths have been falling, due in large measure to the accessibility and affordability of HIV treatment. The number of new HIV infections has also fallen in many countries around the world. While the reasons for this decline vary widely, antiretroviral treatment is undoubtedly a contributing factor, reducing viral load and, hence, the risk of HIV transmission. This progress has led to discussions on the possibility of ending new HIV infections, something unimaginable just 10 years ago.
We may be able to reduce the number of new HIV infections in the world to fewer than 500,000 by 2020, and to fewer than 200,000 by 2030, which would end the AIDS epidemic as a public health threat. Using 2010 as a baseline, these numbers would signify a 75% reduction in new HIV infections between now and 2020 and a 90% reduction by 2030. Meeting these targets will require specific, high-impact HIV prevention measures, testing, treatment, programs to fight discrimination, and an unbreakable commitment to respect protect, and promote human rights.
Nonetheless, despite these significant global advances, Latin America and the Caribbean have not seen a substantial decline in new infections. In fact, there was an increase in 2015, compared to 2013 and 2014. A high incidence of HIV persists among key populations—especially among MSM and among transgender women.
Reducing the incidence of the disease will require strengthening various aspects of HIV prevention and the implementation of combination prevention packages that offer a range of high- impact HIV prevention measures of proven effectiveness that are tailored to local epidemics.
HIV prevention in the spotlight is the product of a multisectoral consultation involving the national AIDS programs of the countries of the region, international cooperation agencies, civil society, and people living with HIV, who have contributed their knowledge and experiences to the discussion. With the valuable information obtained from different sources, this publication presents a joint analysis by PAHO/WHO, UNAIDS, and civil society of the status of HIV prevention efforts and the progress made toward meeting the national and regional prevention targets set by the Latin American and Caribbean countries within the framework of the 2015 Call to Action issued in Rio de Janeiro.

It also presents examples of combination HIV prevention measures and highlights some common challenges, such as inadequate investment and resistance to meeting the specific needs of young adults, adolescents, and key populations in connection with their sexual and reproductive rights, while offering recommendations to address these issues.
The combination prevention approach described herein is fundamental. Countries must recommit to this type of action and seriously examine the importance of targeting interventions to key populations and the need to promote the integration and intensification of HIV prevention programs, while improving their performance and broadening their scope.
A multisectoral commitment, close collaboration with communities, and investment in sustainable prevention are essential if regional agreements are to be transformed into country action. As this publication demonstrates, the prevention targets for implementing the Fast-track Strategy at the regional level can be met if a greater return on each dollar invested can be ensured through efficient investment using a location population approach tailored to the characteristics of each epidemic.
Good practices include the successful interventions of the Global Fund to Fight AIDS, Tuberculosis, and Malaria, targeted to the key populations and described in this publication.
Let us not miss this opportunity to end new HIV infections and improve people’s lives overall, thereby contributing to the realization of the 2030 Agenda for Sustainable Development. AIDS has not ended, but it can end. HIV prevention in the spotlight will be an excellent tool for steering us in the right direction.
Dr. César Antonio Núñez, Director
Regional Support team for Latin America and the Caribbean UNAIDS
The Pan American Health Organization (PAHO) and the Joint United Nations Program on HIV/AIDS (UNAIDS) would like to thank the managers, coordinators, and directors of the national HIV/AIDS and STI programs of Latin America and the Caribbean, their teams, and the national representatives of UN agencies and civil society organizations for their collaboration in data collection and active participation in the national consultations.
This publication was prepared by Mónica Alonso González (PAHO), Javier Hourcade Bellocq (PAHO consultant), Maeve B. Mello (PAHO), and Alejandra Corao (UNAIDS). We thank the following individuals for their contributions to the publication and data collection: Massimo Ghidinelli (PAHO), Bertha Gómez (PAHO), Chen-Ling Hsieh (PAHO), Sandra Jones (PAHO), Diego Postigo (UNAIDS consultant), Pilar Ramón-Pardo (PAHO), Mary Ann Seday (UNAIDS), Héctor Sucilla Pérez (UNAIDS), Giovanni Ravasi (PAHO), Elizabeth Rodríguez (PAHO), Marcelo Vila (PAHO), and the PAHO HIV focal points in the Member States. Our thanks go also to Nasim Farach of the U.S. Centers for Disease Control and Prevention (CDC) and our colleagues in the Secretariat of the Global Fund to Fight AIDS, Tuberculosis, and Malaria as well as the Pan Caribbean Partnership against HIV/AIDS (PANCAP).
The governments of Latin America and the Caribbean (LAC) have made a commitment to putting an end to the AIDS epidemic by 2030. This commitment is aligned with the Political Declaration on HIV and AIDS issued by the United Nations General Assembly in June 2016, with specific targets set in Latin America for 2020 and 2030.
Within this context, the purpose of this publication is to highlight the efforts and challenges to preventing infection with the human immunodeficiency virus (HIV) in LAC through a critical review of the HIV prevention measures adopted by the health sector. The report was prepared with a participatory multisectoral approach involving the compilation of published data and additional data collection through questionnaires and both face-to-face and virtual consultations.
The review and recommendations focus on the health sector and three key populations: female sex workers (FSWs), transgender women, and gay men and other men who have sex with men (MSM).
This report is particularly relevant and timely, because the number of new HIV cases in LAC has remained the same as it was in 2010— that is, approximately 120,000 new infections each year—and the number of new infections in adult males is estimated to have increased between 2010 and 2016. Furthermore, in 2016, young men between the ages of 15 and 24 continued to account for one-third of all new HIV infections.
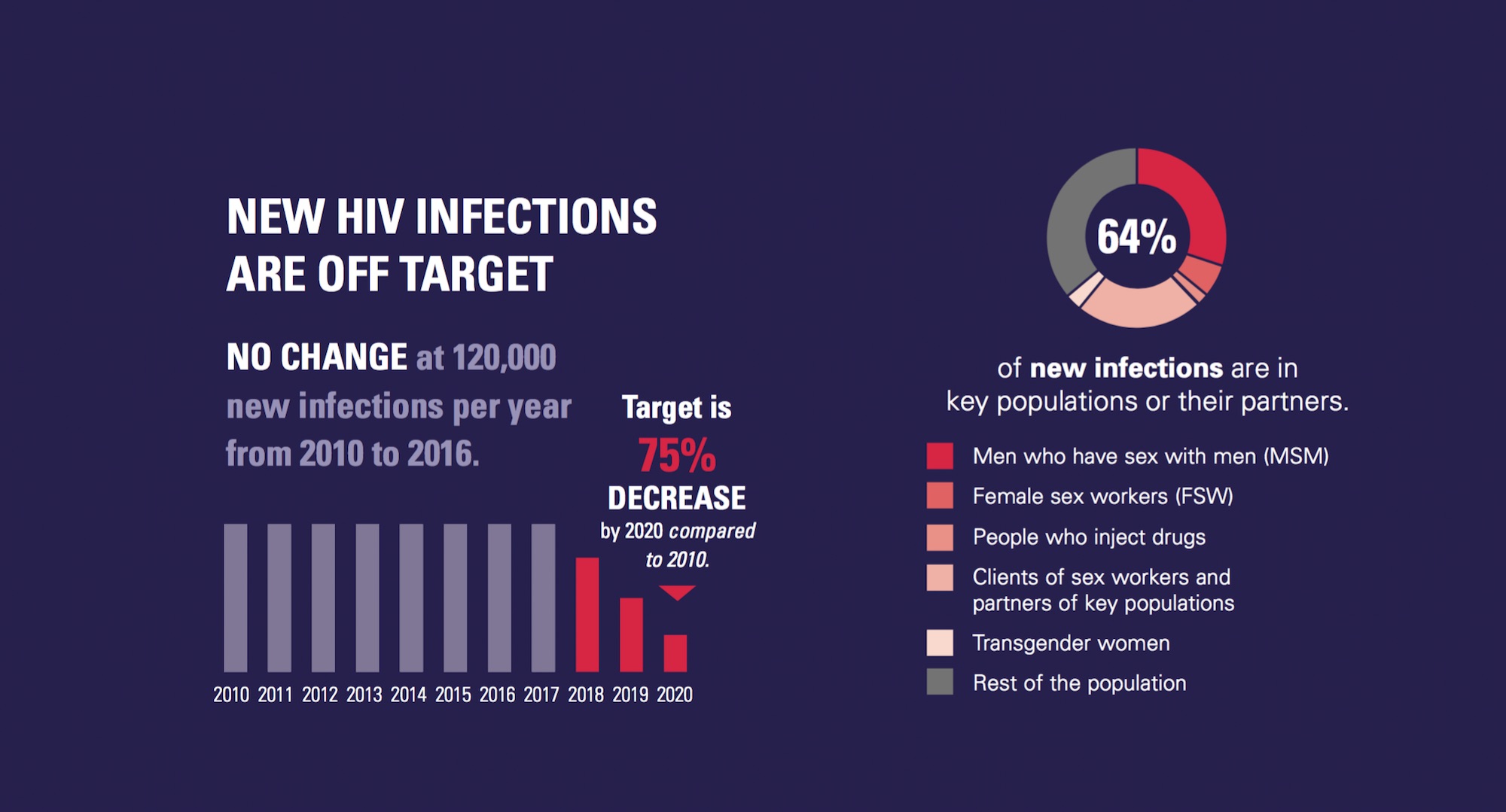
In light of this picture, “combination prevention” is a new approach being promoted to reduce the number of new infections. It combines biomedical and behavioral interventions with interventions that foster an enabling environment to overcome access barriers to health and prevention services.
LAC has made progress in the diagnosis of people with HIV who know their serological status. In 2016, 81% [58%-89%] and 64% [51%-74%] of people with HIV in Latin America and the Caribbean, respectively, knew their serological status. However, delays are still observed in access to diagnosis and health services. An estimated one-third of persons newly diagnosed with HIV were detected late, an indicator that has not improved in the past three years.
Currently, except for the Bahamas, no country offers the complete package of specific interventions for HIV prevention recommended by the World Health Organization (WHO). For example, the data show very limited provision of pre-exposure prophylaxis (PrEP) in LAC, especially for the key populations. Two more countries plan to introduce PrEP in their national public programs in 2017, and seven more are planning pilot projects to implement it.
Every country in LAC offers post-exposure prophylaxis (PEP) that meets two of the three criteria recommended by WHO. Only one- third of the countries also meet the criterion of providing prophylaxis if someone needs it to protect against the risk of transmission during consensual sex.
The regional median for condom use among MSM in their most recent sexual contact is 63%; among FSWs, 80%; and among transgender women, 88%. There has been no apparent increase compared to the baseline, but there has been an increase in availability of information on transgender women. However, according to the information provided by some key individuals from civil society, the number of condoms and amount of lubricants distributed to the key populations are still insufficient to meet their needs, and it is believed that proper and systematic use of these items may be lower than the data report. Furthermore, the sustainability of this intervention is not guaranteed, since only one-third of the countries report purchasing condoms with their own resources; the remaining countries use resources that come largely from two international donors (the Global Fund to Fight AIDS, Tuberculosis, and Malaria, and PEPFAR).
The diagnosis and treatment of sexually transmitted infections (STI) is an essential aspect of HIV prevention. Data show an increase in STIs in the key populations of some LAC countries. These populations continue to exhibit a high burden of syphilis, which ranges from 1% to 27% in the case of gay men and other MSM, and from 0.5% to 14% in FSWs. In this regard, although 88% of the countries report having STI treatment guides, only slightly more than half of them (59%) follow the WHO recommendations. Furthermore, while the data point to an increase in gonococcal resistance to antimicrobial drugs, only 36% of the countries systematically monitor this resistance to support treatment decisions. Finally, the reporting of active syphilis, which is important for detecting outbreaks and taking steps to combat them, is not compulsory in all the countries (only 89% require it).
The majority of national HIV programs report that training and awareness activities are conducted to attend to key populations. However, the effectiveness of these efforts is not monitored and only rarely is civil society involved in them. Stigma and discrimination continue to fuel the HIV epidemic in LAC, particularly in the key populations.
As part of the targets for eliminating AIDS by 2030, the governments have made several commitments, such as allocating one-quarter of the total HIV budget to prevention and ensuring that at least 30% of service delivery is community-run. However, ensuring the sustainability of the intervention package for the key populations and maintaining a significant level of civil society engagement continues to be difficult, since 82% (27 out of 33) of the countries in LAC depend on international funding to carry out prevention activities in the key populations, and only 60% of the countries (15 out of 25) have resources from their national budget to finance civil society initiatives. Furthermore, service delivery to the key populations, as part of integrated health networks, is limited to a few urban areas, and many countries do not have community- run services.
A significant proportion of people in the key populations have access to prevention services, thanks to financing from the Global Fund and other bilateral cooperation, such as that of the United States. This means that a detailed plan for transitioning toward the national sustainability of HIV prevention in the key populations is necessary and shows the high degree financial dependence of a large number of countries in LAC.
In 2016, the number of new HIV infections in LAC was estimated at roughly 120,000 [98,000-140,000]. Since 2010, the decline in the number of new infections has slowed and, in fact, in 12 countries it is estimated to have increased (1). These figures paint a picture in which the commitment to a 75% reduction in new HIV infections by 2020 remains a distant objective.
In order to help countries end the AIDS epidemic by 2030, the Joint United Nations Program on HIV/AIDS (UNAIDS) has developed a strategic framework called the “Fast-track Strategy to End AIDS” (2). Implementing this approach implies setting ambitious targets, substantially increasing current investment, and accelerating the delivery of high-impact HIV prevention and treatment services. At the 2016 World Health Assembly, the Member States of WHO approved the Global health sector strategy on HIV 2016-2021, which defined how the health sector will contribute to meeting these targets by 2030.
In 2014, the 90-90-90 targets were adopted in LAC to guarantee the continuity of HIV treatment. It was recognized that a greater number of synergistic measures were required to reverse the increase in new HIV infections and the AIDS epidemic by 2030. Thus, in August 2015, at the Second Latin American and Caribbean Forum on the Continuum of HIV Care, held in Rio de Janeiro (Brazil), countries of the LAC endorsed the conceptual framework for combination prevention and the regional HIV prevention targets (3) (Table 1).
This publication aims to help the countries of the region rapidly accelerate the improvement and expansion of HIV prevention. It presents a critical analysis of the HIV prevention measures adopted by the health sector to encourage dialogue and national and local decision-making for HIV prevention. The report focuses primarily on three of the region’s key populations: gay men and other men who have sex with men (MSM), female sex workers (FSWs), and transgender women.
Table 1 / Regional HIV prevention targets in Latin America and the Caribbean and situation in 2016
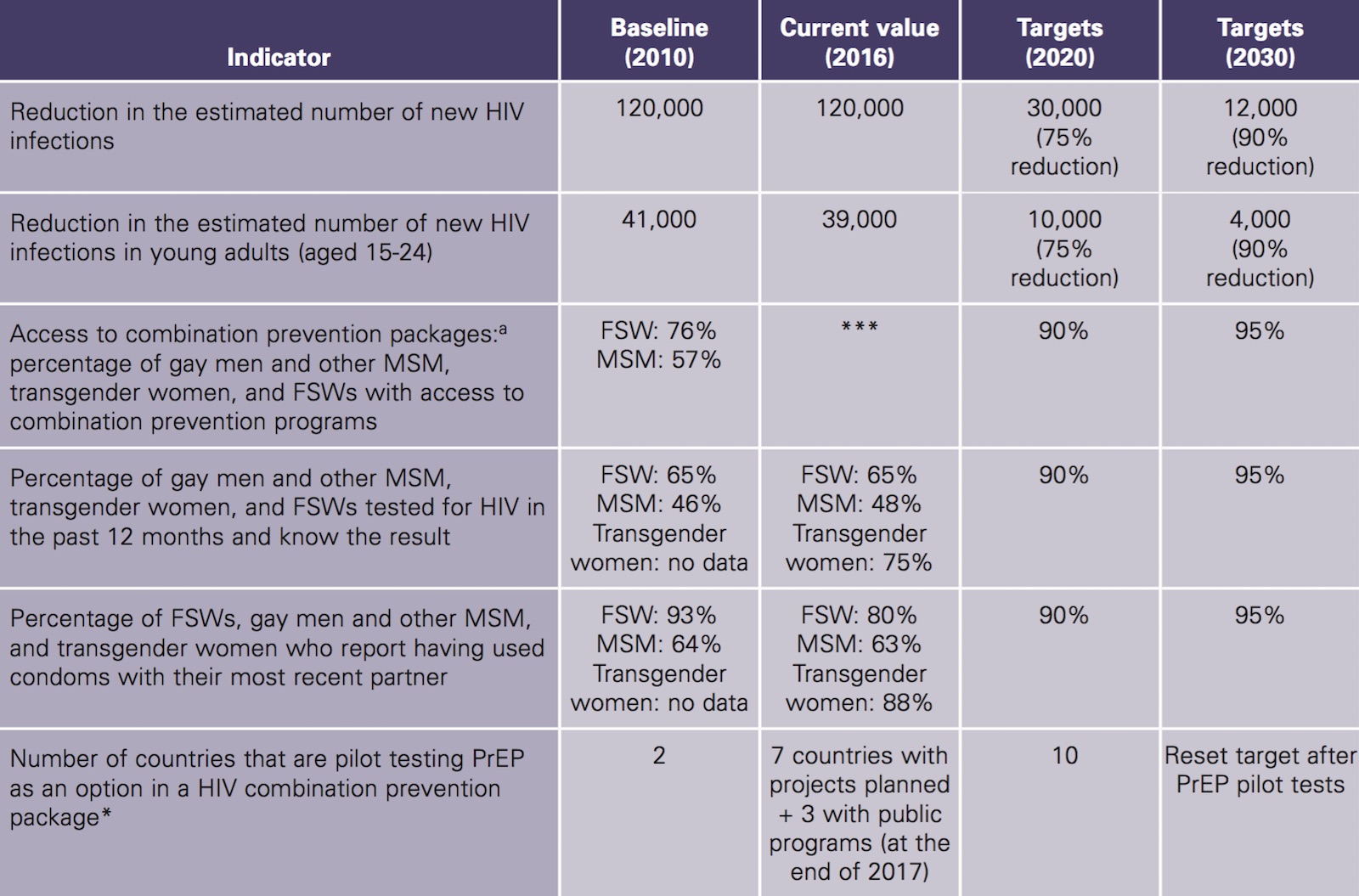
Source: For the 2016 values: UNAIDS, Spectrum estimates corresponding to 2017 (rounded). Notes: Subregional prevention targets can be consulted in Table 1 of the Annex. MSM: men who have sex with men. FSW: female sex workers; PrEP: pre-exposure prophylaxis. a: Appropriate and tailored to the local and cultural context. *** The GARPR indicator has changed; thus, no country-level information is currently available to measure it.
Combination HIV prevention is an approach initially proposed by the United States in the President’s Emergency Plan for AIDS Relief (PEPFAR) and subsequently adopted and expanded in 2009 by the UNAIDS HIV Prevention Reference Group (4). Some years later, it was updated in the report Fast-tracking combination prevention (5).
UNAIDS defines combination prevention programs as rights-, evidence-, and community-based programs that promote a combination of biomedical, behavioral, and structural interventions designed to meet the HIV prevention needs of specific people and communities.
Their goal is to reduce the number of new infections through activities with a greater sustained impact. Well-designed combination prevention programs should be tailored to national and local needs, based on epidemiological information. Programs should also concentrate resources on combining activities where they are most needed. Structural interventions make it possible to create an enabling environment for the synergistic preventive action of the biomedical and behavioral components.
Source: UNAIDS. Combination HIV Prevention: Tailoring and Coordinating Biomedical, Behavioral and Structural Strat- egies to Reduce New HIV Infections. UNAIDS Discussion Paper. Geneva; 2010.
Affected communities should be fully involved in these programs, mobilizing community, private sector, and government resources to achieve the necessary participation, coverage, and continuity (Table 2).
In this context, WHO has recommended some essential health sector interventions for the HIV response targeted to the key populations, known as the “comprehensive package of interventions for key populations” (Table 3).
Table 2 / The three areas addressed in combination prevention
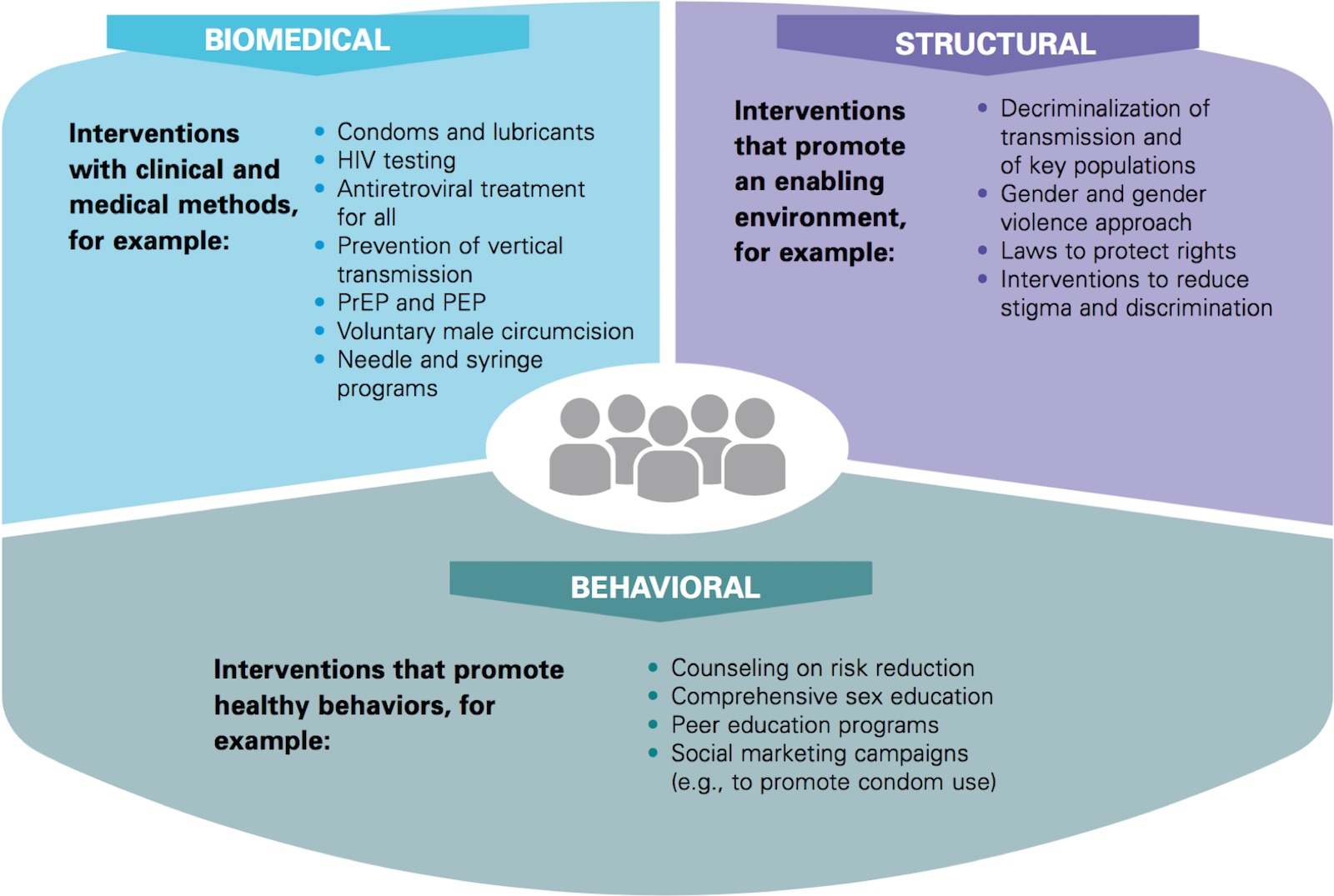
Source: Adapted from the International HIV/AIDS Alliance. An advocacy brief for community-led organisations: Advancing combination HIV prevention; 2016. Available from: http://www.aidsalliance.org/
Table 3 / Comprehensive package of HIV prevention interventions for key populations according to the World Health Organization, 2016

Source: WHO. Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations. 2016 update. Geneva; 2016.
For the analysis in this report, the indicators listed below have been selected, using the combination prevention approach and essential health sector interventions for HIV prevention as a framework, with emphasis on the key populations, regional prevention targets, and the indicators reported at the international level (GARPR/GAM):
In addition to these indicators, given the great importance of the structural component of combination prevention, a brief analysis is included of this component in LAC, focusing on a review of laws, policies, and practices, the reduction of stigma and discrimination, community empowerment, and violence prevention.
Information Sources
The main source of quantitative information was the 2017 country reports for global AIDS monitoring (GAM).
Other sources of information include
An estimated 120,000 [98,000- 140,000] new HIV infections were observed in LAC in 2016, a figure similar to that of 2010.
New HIV infections in Latin America and the Caribbean have trended downward in the past 16 years. Nevertheless, new infections have plateaued since 2010 (with 120,000 new infections that year), although there was a slight decline in 2015 and 2016 (Figure 1). This suggests that LAC is off track in meeting the established global and regional targets of a 75% reduction in new HIV infections by 2020 (Table 1).

Figure 1 / Trend in estimated new HIV infections in Latin America and the Caribbean, 2000-2016
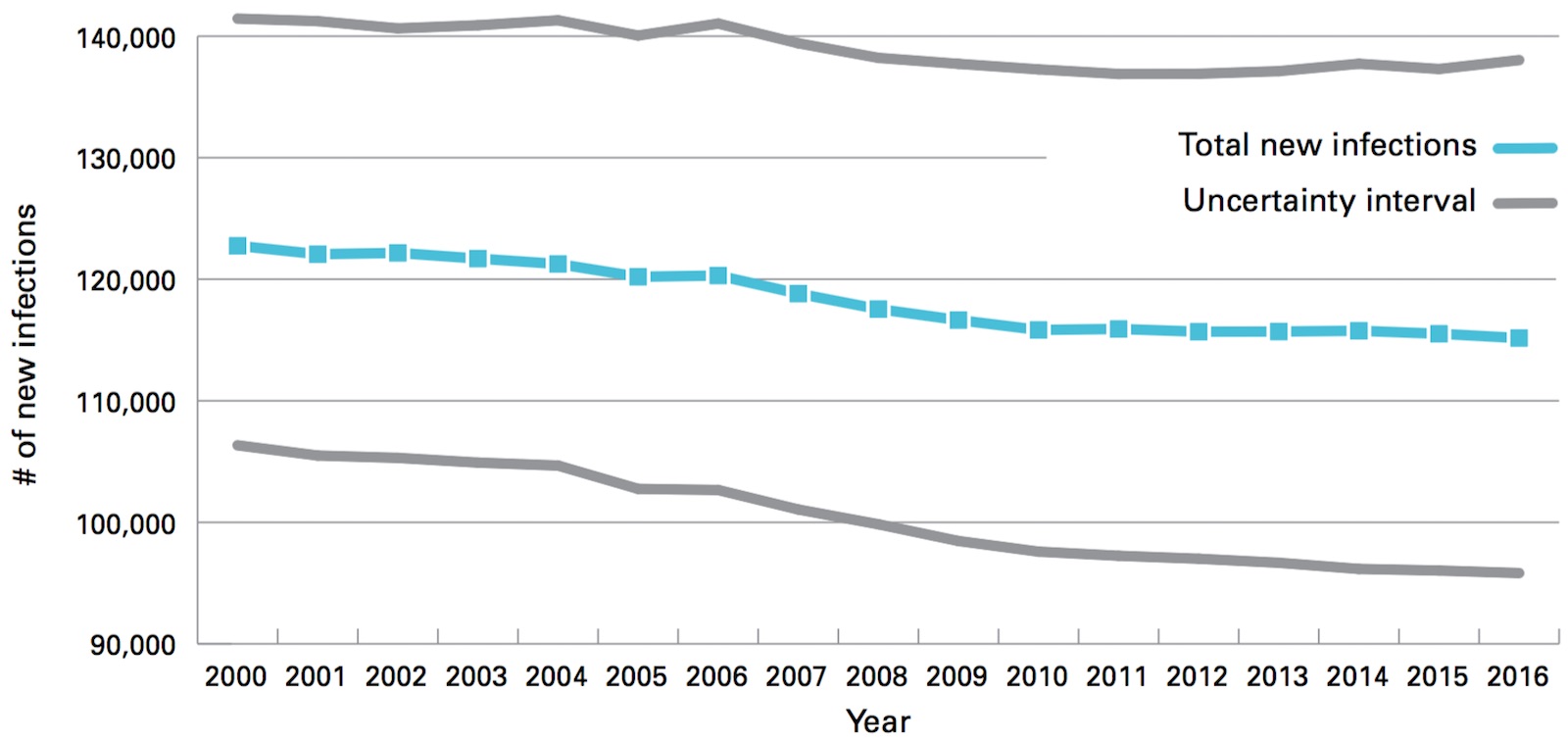
Source: UNAIDS. Spectrum estimates; 2017. Note: Estimates have been rounded.
Few countries have seen a clear decrease in new infections since 2010 (e.g., Colombia, El Salvador, and Nicaragua), while in most countries the trend is steady or even increasing (Table 4). Among males over the age of 15, there was an increase in new infections in the Caribbean from 2010 to 2016 (an 8% increase), while the trend in Latin America was relatively stable (a 2% increase) (Figure 2).
Table 4 / Classification of countries by trends in new HIV infections, Latin America and the Caribbean, 2010-2016
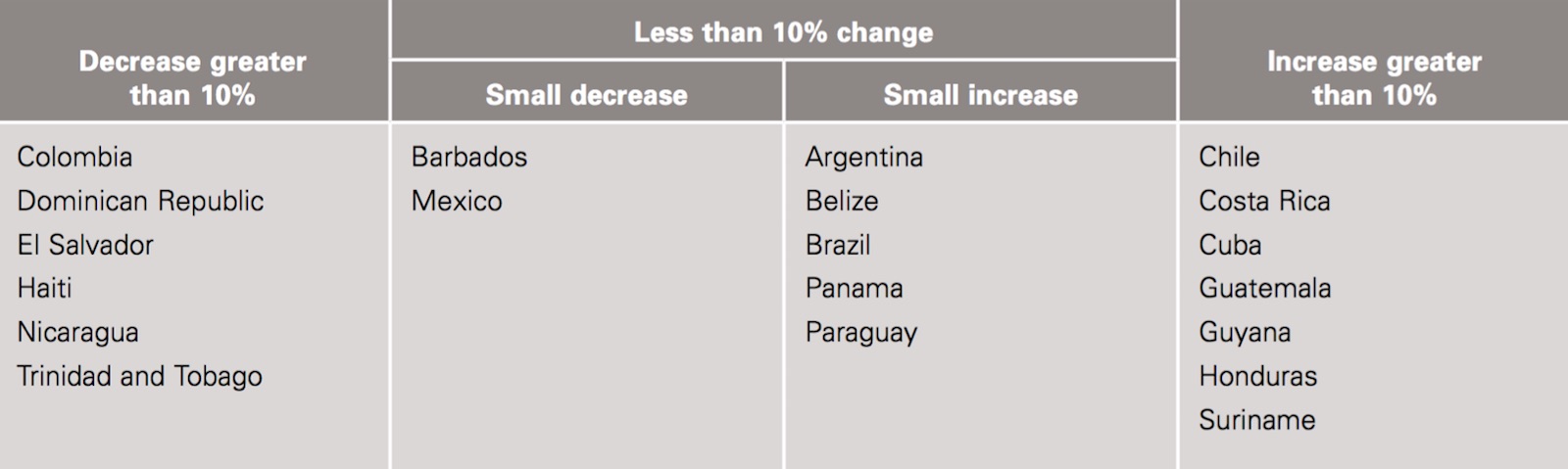
Source: UNAIDS Spectrum estimates, 2017.
Figure 2 / Distribution of estimated new HIV infections among adults (15+) in the Caribbean by sex and year, 2010-2016
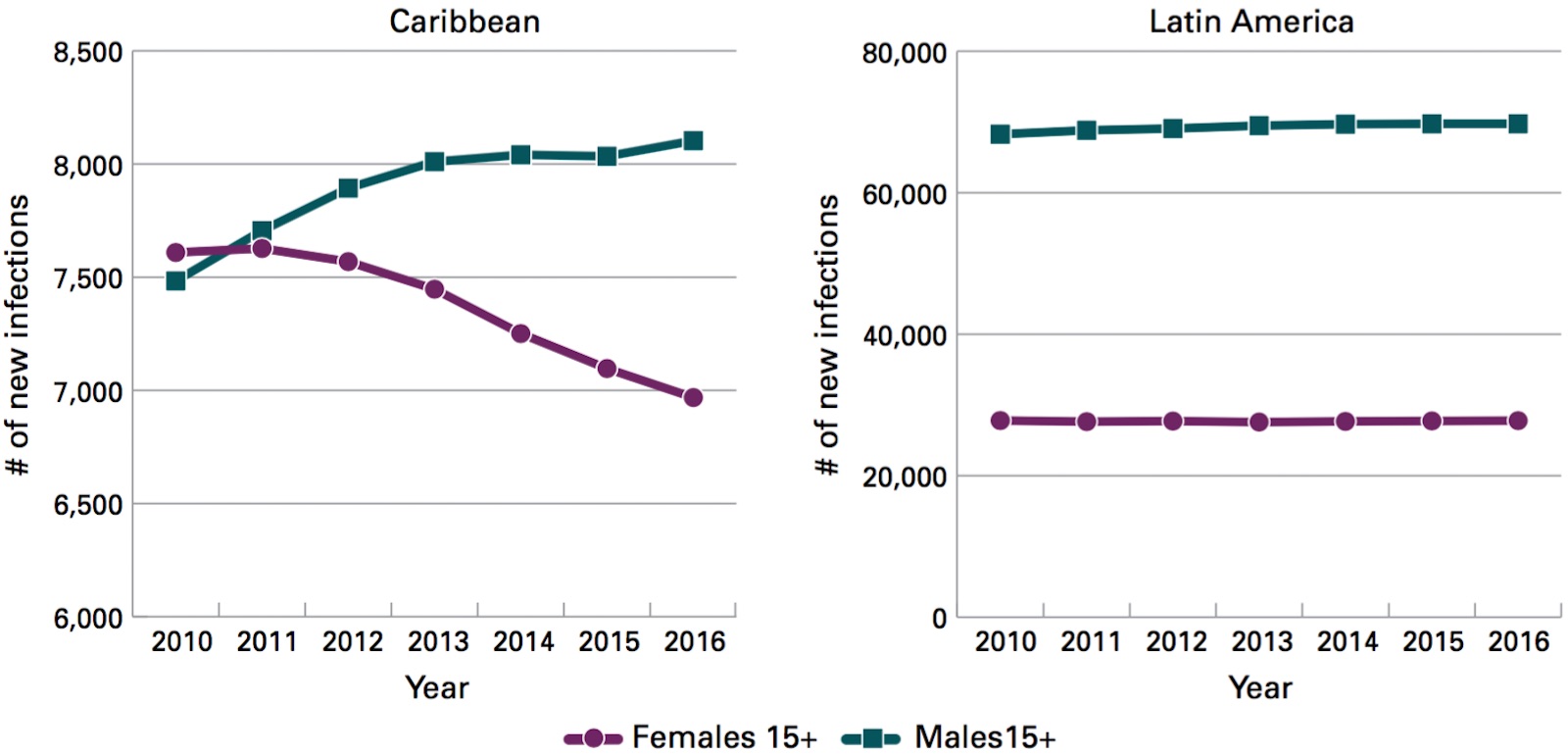
Source: UNAIDS Spectrum estimates, 2017.
Males over the age of 15 accounted for 70% of all new infections in Latin America and 51% in the Caribbean.
In contrast, among females in the same age group, the data show a decline in new infections in the Caribbean (an 8% decline) during the same period. In 2016, in Latin America, males over the age of 15 accounted for 70% of all new infections in Latin America and 51% in the Caribbean. Notably, Haiti is the only Caribbean country with more new infections in females than males (28% more).
Males and females aged 15-24 accounted for one-third of the total estimated population with new HIV infections in both Latin America and the Caribbean in 2016 (Figure 3).
Figure 3 / Distribution of new HIV infections by age group in Latin America and the Caribbean, 2016

Source: UNAIDS Spectrum estimates, 2017.
In this age group, females accounted for a high percentage of the new infections in the Caribbean, while males had two-thirds of the new infections in Latin America.
The regional target is a 75% reduction in new infections in young people by 2020. In the past six years, there has been a 5% decrease in new HIV infections among those aged 15-24 (3% in males and 5% in females) (Table 1).
The number of new infections in young women aged 15-24 in the Caribbean fell by 10% from 2010 to 2016. Among males in the same age group, new infections in that period remained stable (increasing by around 1%) (Figure 4).
Figure 4 / Estimated new infections in young people aged 15-24 in Latin America and the Caribbean, 2010-2016

Source: UNAIDS Spectrum estimates, 2017.
In order to meet the HIV prevention needs of individuals and communities, governments should take full advantage of high-impact interventions supported by evidence and based on the essential rights and needs of each community. They should offer a range of services that individuals will use as their particular needs and situation dictate. These interventions, focused on the aforementioned key populations, (a) include:
National programs and civil society organizations offer a variety of interventions that are not necessarily standard.
The percentage of countries indicating that they have policies for public delivery of these interventions is high in the case of HIV testing and counseling, STI diagnosis and treatment, sex education, and the distribution of condoms. However, public policies are deficient with respect to other services, such as PEP for the key populations, and PrEP and ART for all, regardless of the CD4 count (Table 5).
With the exception of the Bahamas, no country in LAC offers all the recommended interventions to all the key populations, although Brazil is expected to have all the combination prevention interventions by the end of 2017 with the start of its PrEP program in the public health sector. In addition, Barbados is launching an initially small-scale public PrEP program, and the Bahamas has plans to further expand PrEP. The existence of public policies that offer the combination prevention interventions and other related services is the first step toward ensuring access (later chapters examine service coverage and access barriers).
a) The key populations considered in this publication are female sex workers, gay men and other men who have sex with men, and transgender women.
b) WHO recommends antiretroviral treatment (ART) for all adults with HIV, regardless of their clinical status or CD4 count (strong recommendation, medium-quality evidence). Offering treatment to all based on this recommendation is what we call “ART for all” in this report.
Table 5 / Percentage of countries with public policies for delivery of the HIV prevention services recommended by WHO, by key population and selected services
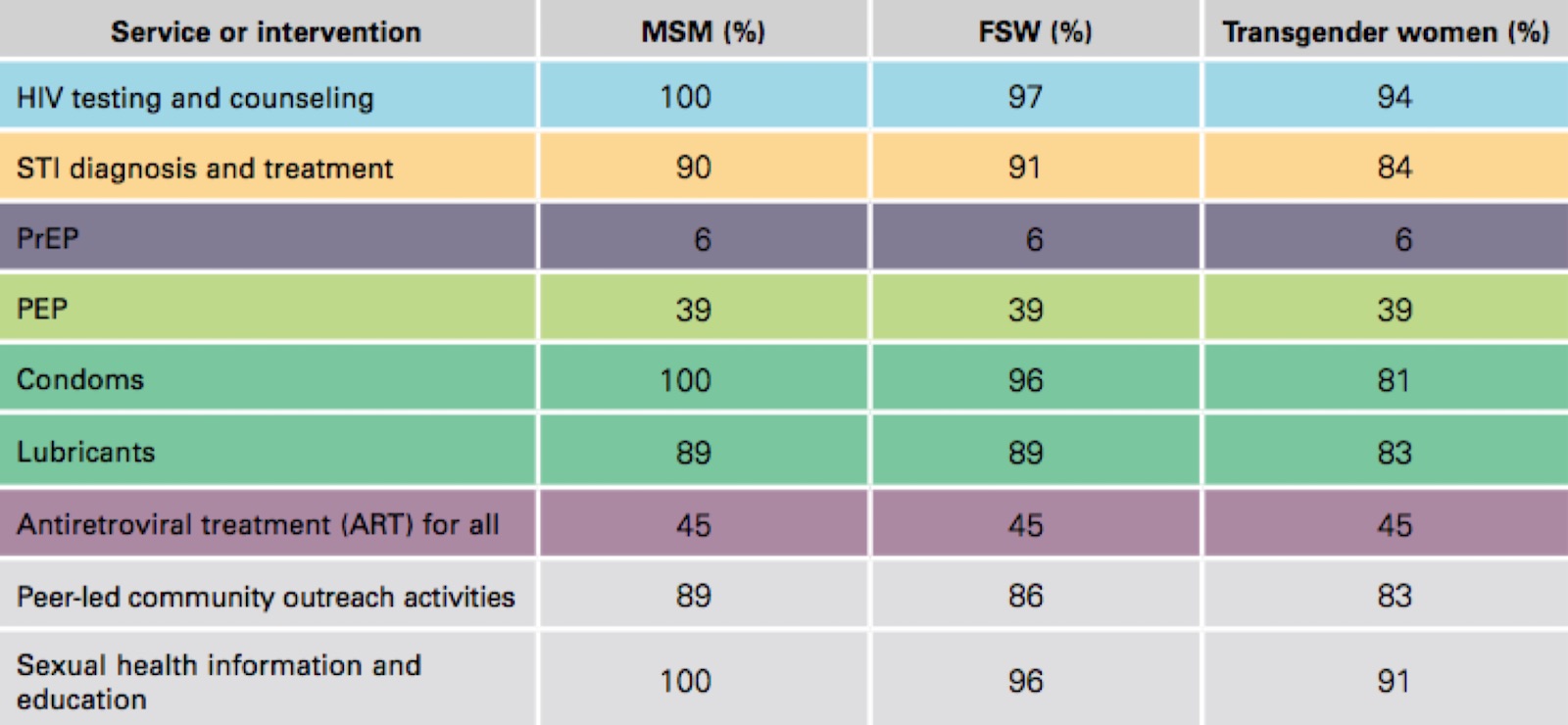
Source: PAHO. Country responses to the HIV Prevention Survey, May 2017. Note: Percentages based on the response of 31 or 33 countries as of July 2017. ART: antiretroviral treatment; MSM: men who have sex with men; PrEP: pre-exposure prophylaxis; PEP: post-exposure prophylaxis; FSW: female sex workers.
The majority of countries offer peer-led community outreach interventions, as well as sexual health information and education. The peer-led community outreach interventions are provided largely by nongovernmental organizations that work with the key populations inside and outside the health services.

of the health sector for the prevention of HIV infection
HIV testing and counseling. Nearly all LAC countries offer HIV testing specifically to the key populations. However, some countries lack specific services for these groups. For example, Saint Vincent and the Grenadines does not have interventions with testing that specifically target FSWs or transgender women, and Haiti does not offer testing to transgender women (these services are part of the packages of services for MSM).c With regard to HIV self-testing, 5 out of 32 countries (19%) indicated that these tests are available on the market. Brazil, however, is the most advanced in implementing this approach in their national policy and plans. Furthermore, throughout LAC, these tests are financed entirely by the user (out-of-pocket expenditure).
A high percentage of countries have public policies that promote these services. However, quantitative and qualitative data and field studies show that not all of them follow the WHO recommendations on systematic STI screening in the key populations. For example, missed opportunities and lack of integrated services have been observed, since 35% of the countries (10/26) report that testing for syphilis and other STIs is not offered when HIV testing is offered to key populations.
The provision of PrEP to key populations is very limited. The regional PrEP target is 10 pilot projects by 2020. That target will soon be exceeded, since by the end of 2017, three countries plan to include or expand its use in their national programs (the latter, in the case of the Bahamas), and seven more are planning pilot projects to provide it (see section on PrEP further on). The regional target will be reviewed before 2020 and a more ambitious target will be set, based on the progress in LAC and the WHO recommendations in this regard.
All the countries offer PEP: a) in cases of work-related or occupational injuries involving a source who is HIV-positive or whose HIV status is unknown, and b) in cases of sexual assault. WHO (6) also recommends that PEP be offered in the case of risk from consensual sex with an HIV-positive sex partner or one whose HIV status is unknown; however, only 39% of the countries offer PEP in this latter case.
The majority of countries report that they distribute condoms to all the key populations, with the exception of Belize, Cuba, El Salvador, Haiti, Saint Lucia, and Trinidad and Tobago in the case of transgender women, and Costa Rica in the case of FSWs (as indicated earlier, services for transgender women are provided by the services for MSM). Lubricants are sometimes not distributed; for example, three countries do not provide them with condoms for MSM or transgender women, and two others do not provide them for FSWs. The majority of the countries do not distribute lubricants along with condoms for the general public or young people (30%; 8 of the 26 countries that provided information). Proper and systematic use of condoms and compatible lubricants is recommended for all the key populations (a strong WHO recommendation) (7). As indicated further on (in the section on condoms), even where public policies for the distribution of free condoms and lubricants are in place, the supply is often insufficient to meet the needs of the key populations.
Roughly half the countries (15/33) in LAC report having adopted the WHO recommendation to offer treatment to all HIV-positive people, regardless of their CD4 count, and 39% (13/33) are planning to adopt this therapeutic criterion. Early HIV treatment improves the patient’s quality of life and is an opportunity to prevent transmission, since a person with an undetectable viral load has a minimal probability of transmitting the virus (8). Nearly 1.2 million people in LAC (162,000 in the Caribbean and over 1 million in Latin America) received ART in 2016, or 100,000 more people than in 2015. In terms of the total population with HIV in 2016, people who received ART accounted for 52% [41%-60%] of the people with HIV in the Caribbean and 58% [42%-72%] of those in Latin America. Nevertheless, it is essential to take into account suppression of the viral load. In 2016, the viral load was eliminated in 81% [64%-94%] and 72% [52%-89%] of the people receiving ART in the Caribbean and Latin America, respectively. While these figures indicate a certain degree of treatment program success, they still represent less than half the population with HIV (34% with suppressed viral load in the Caribbean and 46% in Latin America), which is far from the target of suppressing the community viral load by 72%––the figure required for epidemic control and to meet the 90-90-90 targets.
The Global Fund to Fight AIDS, Tuberculosis, and Malaria finances interventions that are part of the national HIV response in 18 countries in LAC (in 17 of them, targeting one of the key populations). It also provides funds for regional grants, including the one for HIV prevention in the key populations of the eastern Caribbean. In recent years, the Global Fund has recommended that grant applications from countries with concentrated epidemics should focus on effective interventions for prevention in key populations. (d)
All of the 17 countries that have received grants for HIV prevention in the key populations have funds for interventions with MSM; 14 of them have funds for transgender women; and 12, for FSWs. Three countries (Belize, Guyana, and Haiti) do not have HIV prevention programs for transgender women, although this group has access to such interventions through interventions for MSM. Four countries (Belize, Bolivia, Colombia, and Peru) use domestic funds to finance services and interventions for FSWs.
d) All the information analyzed in this section is taken from the Grant Performance Reports that the Global Fund publishes on its website and updates semiannually with the results of the discussion on the monitoring of each of the grants to the countries.
e) For the 2014-2018 implementation cycle.
Among other interventions, the Global Fund invests in prevention packages. In all cases and for all population groups, these packages include various quantities of male condoms, which are provided during behavior change communication activities. Four out of five grants also cover lubricants.
In recent grant applications, all of the countries have had to set targets for the population to be reached by the end the grant period. Based on national estimates of the size of each of the key populations, the experience working with the different groups, productive capacity, and the potential for expanding the interventions during the program implementation period, the country concept notes have indicated the number of people from the key populations that can feasibly be reached in the total population (Table 6 and Table 2 of the Annex).
With respect to the targets for the percentage of the population that can feasibly be reached,e even if all the programs were properly implemented, none of the three subregions would reach 70% of the MSM population with HIV prevention packages. In the case of transgender women and FSW, none of the three subregions would reach, on average, more than 80% of transgender women or FSW with prevention packages (Figure 5).
Table 6 / Percentage of the key populations that each country in LAC defines as reachable, target with respect to the estimated total, and target as a percentage of the reachable population
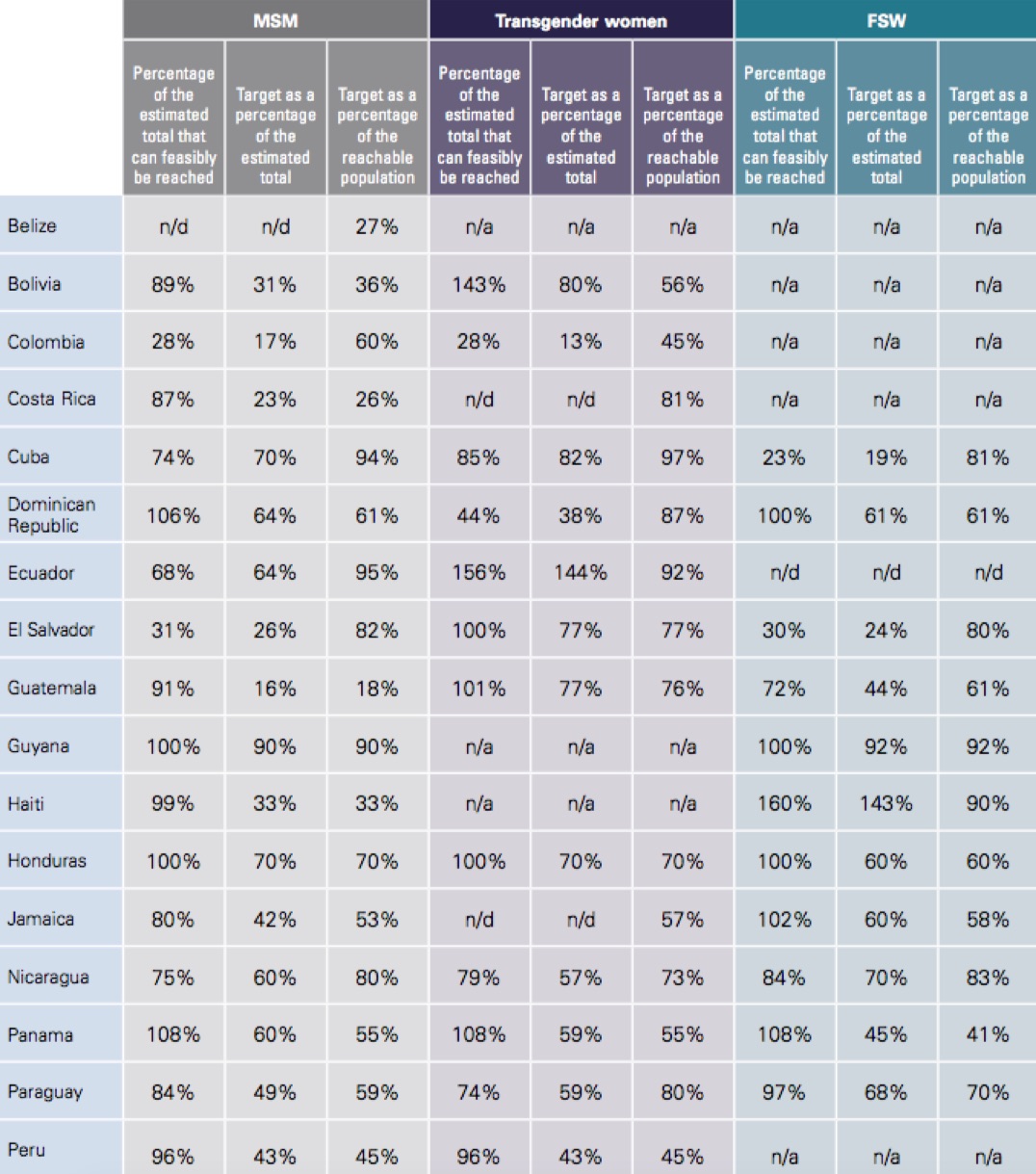
Notes: 2014-2017 financing cycle. MSM: men who have sex with men; FSW: female sex workers; n/a: not applicable; n/d: unavailable.
The 17 countries have an estimated population of 1,158,055 MSM feasible to reach with HIV prevention programs, or 68% of the total estimated MSM population of 1,712,619.f Of these, 448,900, or 38%, had been reached with prevention packages as of December 2016, according to each Global Fund grant. A total of 197,163 (19%) had been offered and given an HIV test.
Of the 78,708 transgender women feasible to reach (83% of the total estimated trans population of 94,522),g 33% (25,568) had been reached with prevention packages and 16% with the HIV test in the 14 countries with grants for this group.
f) Belize does not have estimates of the size of its MSM population.
g) Costa Rica, Cuba, and Jamaica did not provide an estimate of their transgender population in the 2016 GAM.
Of the 341,016 FSWs feasible to reach in the 12 countries, 216,697 (63%) had access to prevention services and 42% received an HIV test.
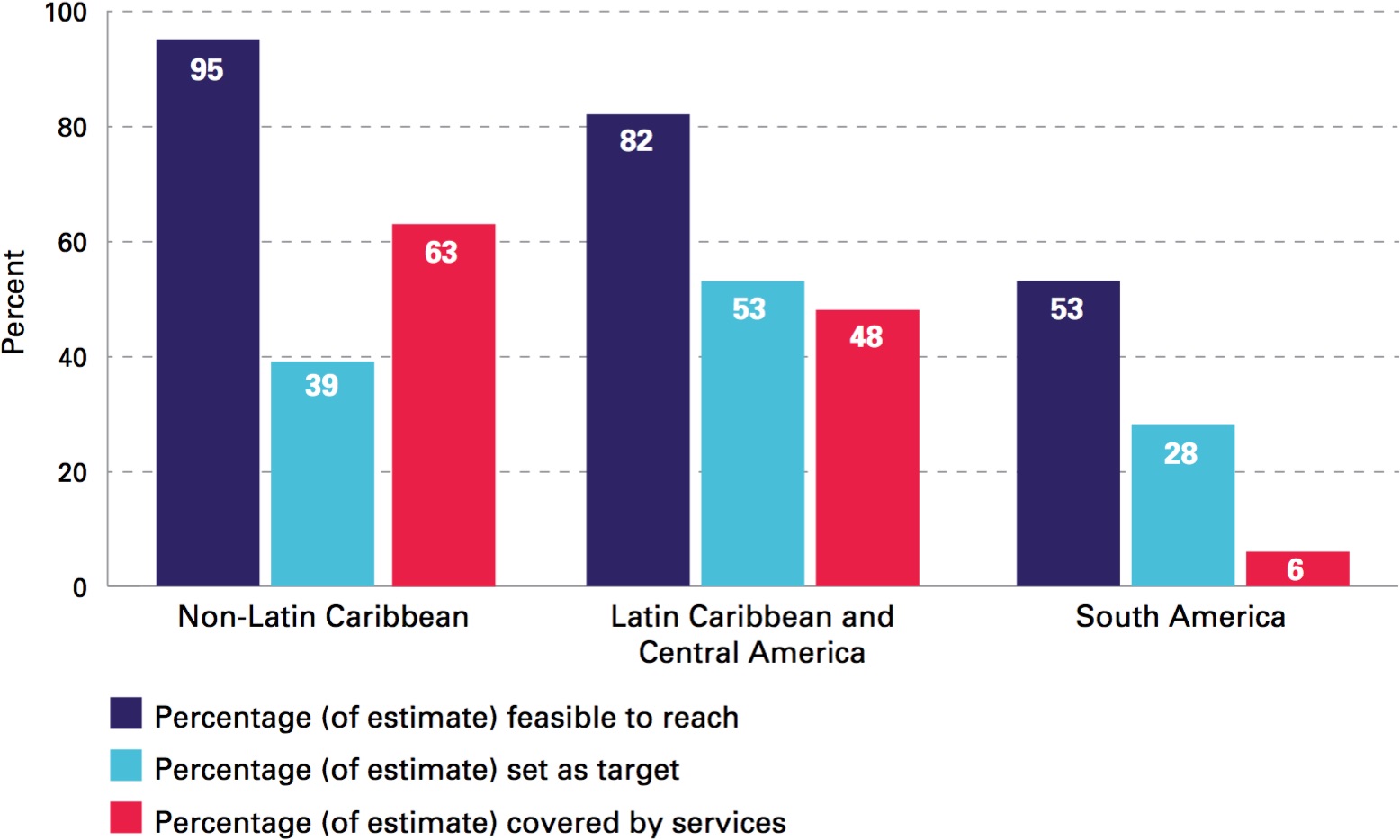
A look at these data by subregion shows that the non-Latin Caribbean countries consider it feasible to reach virtually their entire MSM population with prevention packages, although 39% of this population was set as the target to reach with Global Fund grants. Nevertheless, as of December 2016, 63% of the total had been reached (Figure 6).
Figure 5 / Target of each key population to be reached, based on those that can be feasibly reached, by subregion, 2014-2018 financing cycle

Note: Only interventions financed by the Global Fund. There are no data for transgender women in the non-Latin Caribbean, because only one coun- try has a specific grant for this group; the rest of the countries include these interventions in those for the MSM population. There is no average for FSWs in South America, because only two countries have a grant for this population and only one has data.

© Joshua E. Cogan
A significant proportion of people access HIV prevention measures thanks to financing from the Global Fund. Planning for a transition to national sustainability of HIV prevention measures is needed in three out of four countries in LAC.
Figure 6 / MSM prevention services programming cascade, by subregion, 2014-2017 programming cycle
Similarly, in the case of transgender women (Figure 7), the Latin Caribbean and Central American subregions are where the highest percentage (79%) of the estimated population is feasible to reach with prevention packages. The target was 62% of the total, and as of December 2016, 56% of the total had been reached.
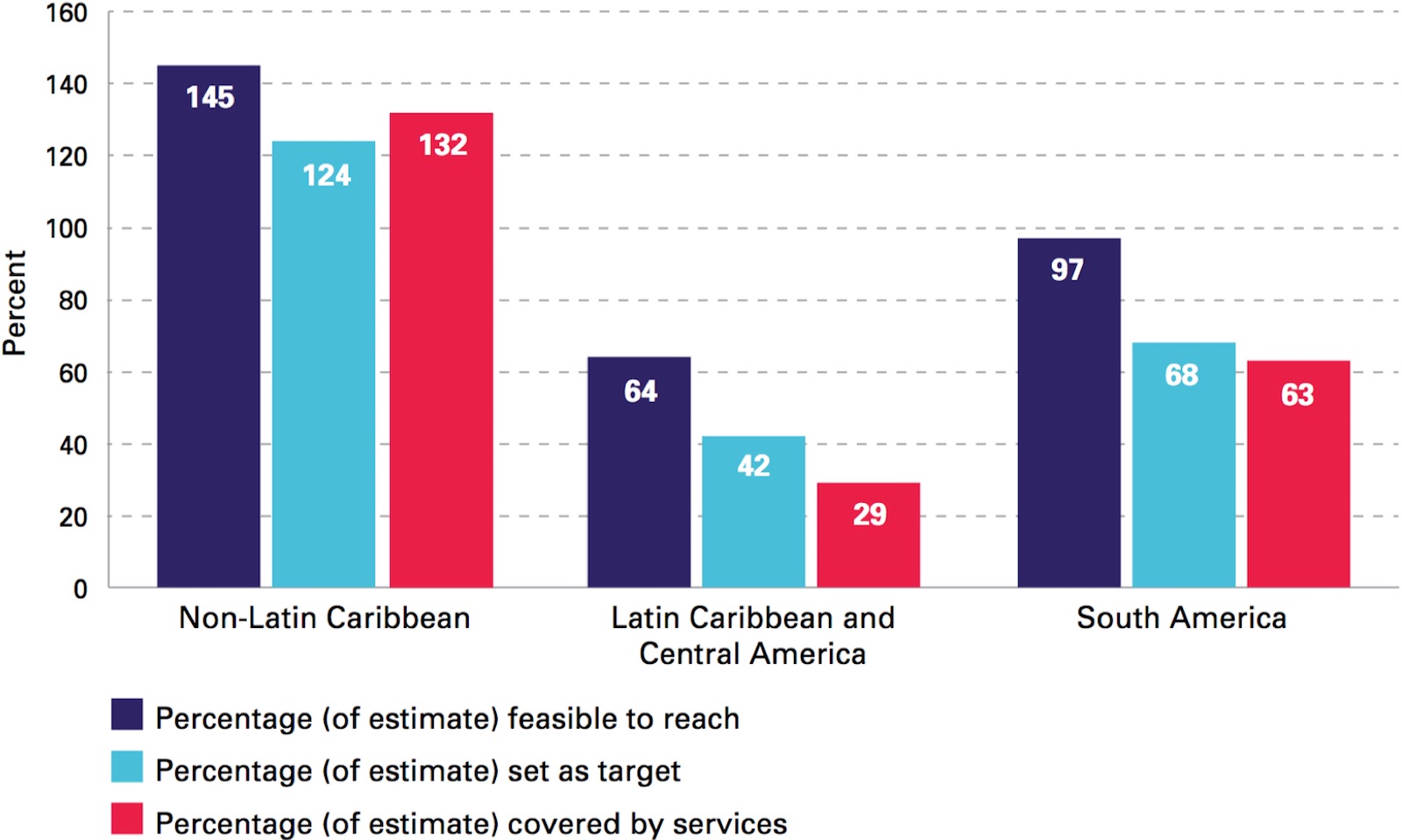
With regard to the FSW population (Figure 8), the estimates of population size reported by the non-Latin Caribbean seem conservative, given that the feasibly reachable population indicated in the Global Fund grants exceeds the figure by almost 50%. The target is 124% of the total, and as of December 2016, 132% had been reached.
The prevention service programming cascades (see Figures 6-8) reveal variability in the estimates of population size between subregions, the population feasible to reach, the targets, and the coverage achieved by the services. The reasons for these differences may be due to
h) The new financing model covers a cycle that began in 2014 and concludes in 2018. Since these are three-year programs, the countries are not all in the same implementation cycle, which affects coverage values.
Figure 7 / Transgender women prevention services programming cascade, by subregion, 2014-2017 programming cycle
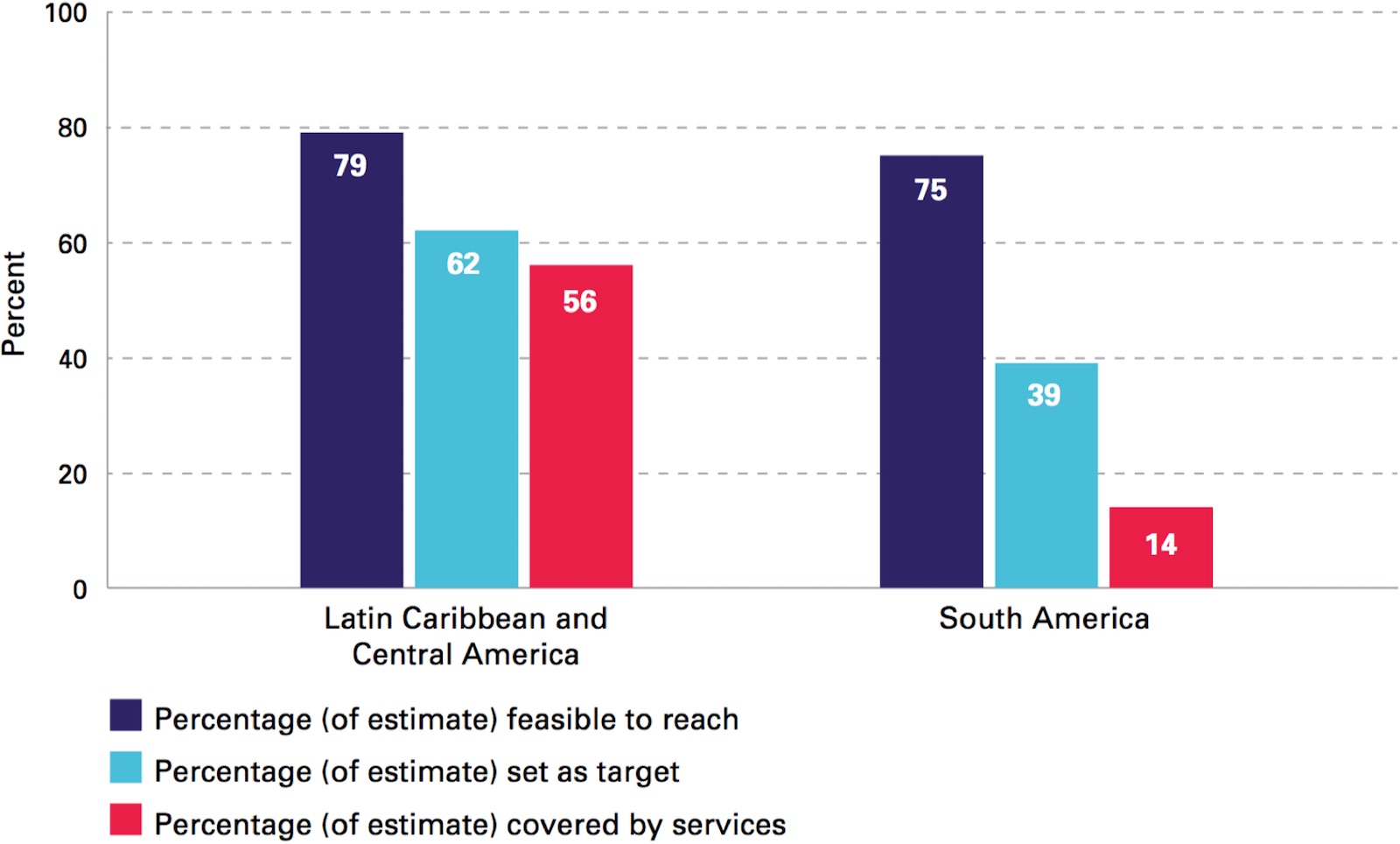
Note: In the non-Latin Caribbean, only Jamaica has individually included it in its grant. Nevertheless, without an estimate of the size of the population, the percentages cannot be calculated.
These cascades also reveal the countries’ dependence on international funds to offer HIV prevention services to the key populations.
The percentage of people from the three key populations reached with HIV prevention packages in the countries varies widely (see Figures 6-8). However, it can be concluded that a very significant proportion of people from the key populations in all the countries have access to HIV prevention measures, thanks to financing from the Global Fund. This situation reveals the need to plan for a transition to national sustainability of HIV prevention measures in three out of four countries in LAC.
Another example of effective services for the key populations are those promoted by the Central American countries with the support of bilateral cooperation from the United States. Thanks to the Sexually Transmitted Infection Surveillance, Prevention, and Control Strategy (known by its Spanish acronym, VICITS), HIV prevention services in the Central American subregion have focused on the needs of the key populations.
Figure 8 / Sex worker prevention services programming cascade, by subregion, 2014-2017 programming cycle
The VICITS strategy is a combination prevention strategy for key populations that offers HIV testing, STI diagnosis and treatment, counseling by specialists, the distribution of condoms and lubricants, peer promotion and accompaniment to HIV treatment and other complementary services, and an information system for the surveillance of epidemiological trends. The ministries of health of Guatemala and Honduras were the first to embrace the strategy, implementing it in 2006. The governments of Costa Rica, El Salvador, Nicaragua, and Panama subsequently followed suit, and VICITS is now being implemented in 47 clinics in LAC, which provided services for 22,616 people in 2016. Access to services, especially by MSM and transgender women, has significantly increased: the number of people reached has risen from the 857 in 2011 to 13,359 in 2016.
VICITS has become one of the most effective strategies for reaching people with undiagnosed HIV and ensuring that they receive treatment. A total of 931 MSM and transgender women in Central America received an HIV diagnosis in 2016 through the VICITS strategy (positivity rate: 10%), a percentage substantially higher than the national prevalence, which is no more than 1% in any of the countries where the strategy is being implemented. Connection to HIV treatment through VICITS is also higher. In Guatemala City, for example, 9 out of 10 people diagnosed with HIV in VICITS clinics in 2016 were connected with the health services within an average of three days, a rate that exceeds the national average by almost 30%. In an effort to improve access by the key populations to HIV treatment, at least seven VICITS clinics offer ART (as of July 2017), and several ministries of health are in the process of decentralizing treatment to new VICITS clinics.
In addition, the VICITS clinic of The Amigos Contra el Sida (Friends against AIDS) group in Guatemala City is conducting Central America’s first PrEP pilot project, and the Ministry of Health of Panama is developing an additional pilot project to offer PrEP in the country’s VICITS clinics, known locally as “friendly clinics.”
The VICITS strategy addresses the stigma and discrimination that the key populations face and trains all health personnel to provide compassionate, high-quality services. VICITS clinics build close ties with the key populations’ community organizations and appoint peer promoters and navigators to promote visits to clinics and connect people diagnosed with HIV with treatment centers. Furthermore, the ministries of health have partnered with local community organizations to conduct VICITS outreach activities. The purpose of this initiative is to offer services outside the customary clinic hours.
Concerning efforts to achieve sustainability, the strategy currently receives funds from the U.S. government. However, the services are provided mainly in government health clinics, and the health care providers are hired by the ministries of health, which also covers the cost of treatment for STIs and the bulk of laboratory reagents.
The VICITS sentinel surveillance system provides information on current HIV and STI trends, condom use, the number of sex partners, and other behavioral indicators in the key populations. These data help to identify the subgroups at greatest risk of infection, provide the information needed to design specific program interventions, and serve as the foundation for HIV and STI indicators in the key populations. They are also a critical tool for supporting domestic and international resource mobilization efforts for the HIV response in the key populations.
Source: Nasim Farach. Central America Regional Office, Centers for Disease Control and Prevention (CDC). Note: The findings and conclusions in this box are an intepretation and do not necessarily represent the official position of the CDC.
The LAC countries have made a commitment to improving access to HIVs testing and people’s knowledge of their HIV status. Three targets have been set: 1) 90% of people with HIV will know their status by 2020; 2) focus efforts on timely access to HIV testing in the key populations, so that by 2020, more than 90% will have been tested in the past 12 months; and 3) reduce late HIV diagnosis to 10% or less (9).
Significant improvements have been made in HIV-positive people’s knowledge of their HIV status in LAC. In 2016, an estimated 81% [58%-89%] of people with HIV in Latin America knew their status and 64% [51%-74%] in the Caribbean. In both cases, improvements were observed over the previous year, when 77% and 57% of such people, respectively, knew their status.
The gaps in access to HIV testing among the key populations are still significant. Furthermore, many countries do not have data on testing for transgender women or FSWs. Some 88% of the countries have at least one figure for this indicator for MSM, 67% for FSWs, and 36% for transgender women. In most of the countries, this target is monitored through behavioral studies in the key populations, from whom data are obtained in some urban centers. Many countries (around one-third, or over 10) have received international financial assistance to conduct these studies.
One out of three diagnoses is late
Figure 9 / Percentage of men who have sex with men (MSM), female sex workers (FSW), and transgender women who have been tested for HIV in the past 12 months in Latin America and the Caribbean, most recent year available

Source: UNAIDS/WHO, Country reports, Global AIDS Response Progress Reporting, 2011-2016, and PAHO, Country responses to the HIV Prevention Survey, May 2017. Note: Data from countries with program data, such as Guyana, Panama, and Peru, have not been included.
The median HIV testing coverage in the past 12 months is 48% for MSM (with figures ranging from 5% in Peru to 19% in the Dominican Republic, and up to 95% or more in Suriname and Saint Kitts and Nevis, according to program data), 65% for FSWs, and 75% for transgender women (with figures ranging from 43% in Colombia to over 95% in Guatemala and Paraguay) (Figure 9 and Table 3 of the Annex).
The regional analysis of this information has limitations, since some countries (Guyana, Panama, Paraguay, and Peru) use data from the health care services. The results are not always representative of all the key populations, and there may be selection and information biases in the data reported, among other limitations.
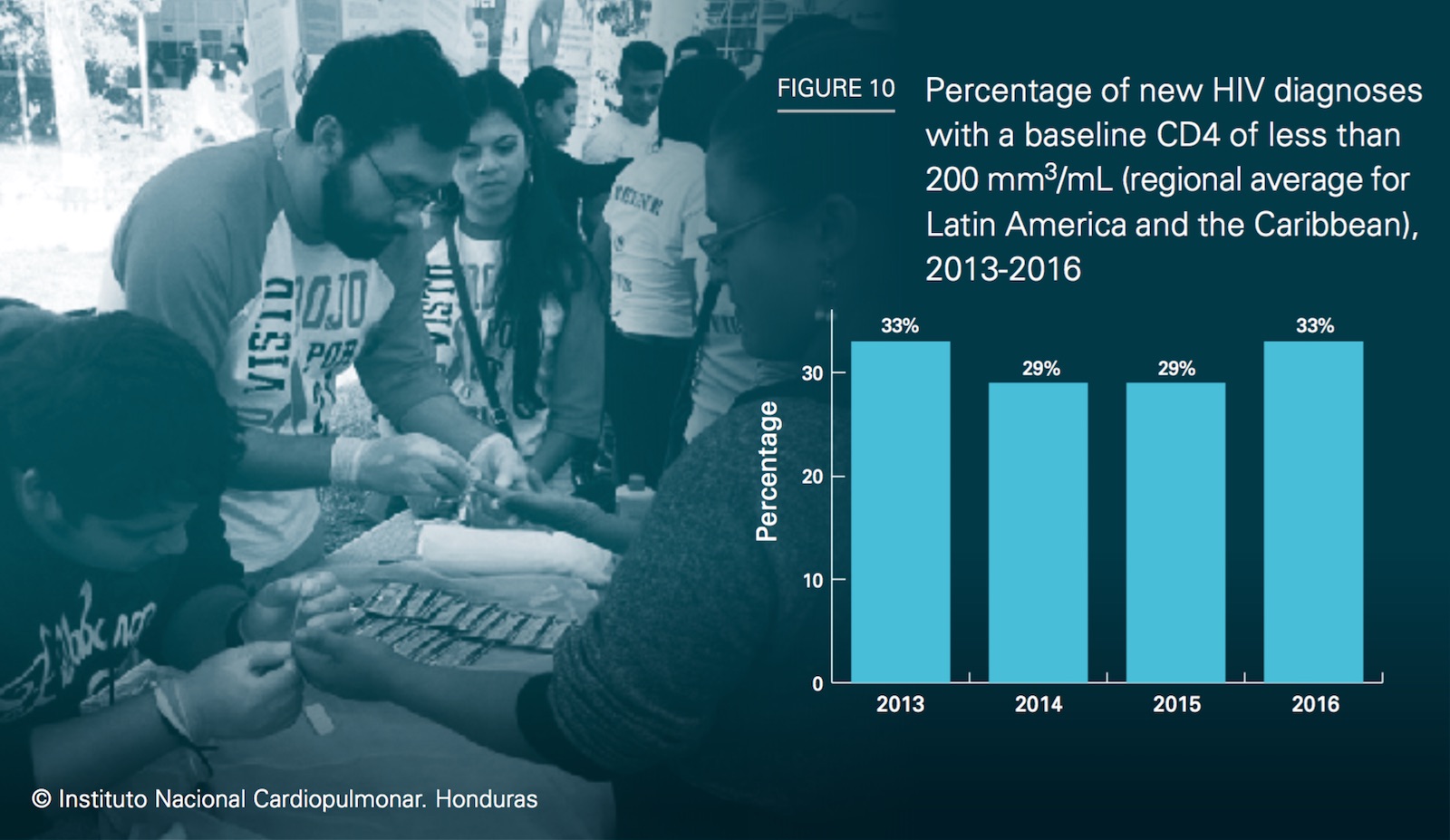
i) The late diagnosis indicator is the percentage of HIV+ people who have a CD4 count of less than 200 cells/mm3 in their first CD4 test.
Another indicator for evaluating the degree of access to HIV testing is late diagnosis.i In LAC, one-third of cases are diagnosed late. The regional average has not changed substantially in the past four years (Figure 10).
Furthermore, in an analysis of the data by country, 59% (13/22) had the same or worse results in 2016, compared with 2015, while 41% (9/22) showed improvements.
Regionally, late diagnosis is more common in men (30% in 2016) than in women (19%). There were no substantial changes in this indicator for men in comparison with 2015. However, an improvement was seen in women (down from 24% in 2015).
In short, these data show that access to testing has improved. However, the gaps are still substantial and access is inadequate. Furthermore, the information systems in many countries do not contain information on testing disaggregated by the key populations.
Source: UNAIDS, WHO. Global AIDS Monitoring (GAM) and Country reports, Global AIDS Response Progress Reporting (GARPR), 2014-2016.
Regionally, late diagnosis is more common in men (30% in 2016) than in women (19%).
This makes it hard to measure inequities in access and timely testing in these populations. The LAC countries face a series of barriers to providing adequate access and testing for the key populations, the most important of which are detailed below.
Note: Based on the results of the national consultations.
j) The WHO recommendations are available from: URL 1 and URL 2
a. Up-to-date algorithms and the use of rapid tests to increase access. Countries such as Chile, Ecuador, Peru, Suriname, and Trinidad and Tobago are modifying their algorithms to optimize the testing process and reduce waiting times to confirm a positive diagnosis. Simplification of the diagnosis algorithms can help yield reliable and timely results.
b. Decentralization of testing and use of diversified strategies to offer the test. Some 68% of the countries report that testing is offered in community centers. Some 43% of the countries (13/30) allow HIV testing to be done by trained individuals who are not health professionals (e.g., Argentina, Dominica, Guatemala, Jamaica, Mexico, and Paraguay). However, in countries that offer testing in community centers, the majority of tests in the country (90%) are done by health centers and only 10% by civil society organizations or private laboratories. That is, the number of tests done by community- based services or civil society organizations is small and is normally in connection with grants from international donors.

© Joshua E. Cogan
c. Distribution of centers that offer testing. In the majority of the countries, these centers are concentrated in large cities. This creates problems for people living in communities far from urban centers.
d. Hours of operation tailored to the needs of key populations. Some 62% of the countries (16/26) offer services with flexible hours for HIV testing, generally provided by civil society organizations. Flexible hours enable the key populations to get tested at times that are more convenient for them— for example, late afternoons or evenings.
e. Use of self-testing. This type of test, which can increase the number of people who know their HIV status, is now on the market in different countries, including the Bahamas, Brazil, El Salvador, Jamaica, Peru, and Trinidad and Tobago. However, no government has yet documented a subsidized cost or using it to expand testing to hard to reach groups or to establish mechanisms to link people with the health services.
In the majority of LAC countries, the age of consent is 18 for young people to seek HIV testing on their own.
f. Legal barriers. The age of consent for a young person to seek HIV testing at the health services on his or her own is 18 in 61% of the countries.
g. Procedures to ensure confidentiality and informed consent. The written informed consent requirement persists in several countries. This can be a barrier to broadening access to HIV testing. WHO has noted that, in most settings, verbal consent is enough to obtain an HIV test (11).
h. Stigma and discrimination. Ninety-two per- cent (24/26) of the countries provide sensitivity training for health workers involved in HIV screening for key populations. However, civil society organizations in 12 countries that par- ticipated in national consultations on HIV prevention reported a lack of sensitivity among these professionals. The factors associated with this situation may be:
According to WHO estimates (12), in 2012, 51 million sexually active people aged 15-49 in the Region of the Americas had an STI, making it one of the regions with the highest burden of disease, along with the African and Western Pacific regions. STIs affect health status because they cause acute disorders such as cervicitis, urethritis, and genital ulcers, in addition to serious complications and sequelae such as ectopic pregnancy, infertility, neurological and cardiovascular disease in adults, neonatal death, premature birth, and blindness or severe disability in infants. They also increase the risk of contracting and transmitting HIV (7). STI diagnosis and treatment is part of the comprehensive package of services provided in combination HIV prevention.
In recent years, the Region has documented outbreaks and increases in the incidence and prevalence of STIs (13). Barbados has reported increases in syphilis in 2013 and 2014, again, especially in men (72%)—percentages that stabilized at high rates in 2015 and 2016 (14).
Sentinel surveillance centers in Guatemala have also reported that positivity for active syphilis in MSM has increased more than 10-fold (from 0.9% in 2014 to 11.6% in 2016). In Mexico, the Institute of Public Health has also reported an increase in syphilis in some states (Yucatán, Campeche, Tabasco, etc.) (15). As in some countries outside the Region, there have been outbreaks of hepatitis A among gay men and MSM in Chile and Brazil, as well as the United States (Colorado and Michigan).
MSM and FSWs continue to exhibit a high burden of syphilis, with rates of 1%-27% in the case of gay men and MSM (Table 4 of the Annex) and 0.5%-14% in FSWs (Table 5 of the Annex), with figures that are higher and, in some cases, similar to the prevalence in pregnant women (Table 6 of the Annex). (k) Considering the high vulnerability of the key populations and their high STI burden, monitoring prevention efforts and their outcomes in these populations should be a priority in LAC.
k) The prevalence of syphilis in pregnant women receiving prenatal care in countries reporting active syphilis, ranges from 0.0% to 2.9%, with a median regional prevalence of 0.8%.
Latin America and the Caribbean are facing a resurgence of STIs in some population groups and an increase in gonococcal resistance to antimicrobial drugs (16). In response to the STI epidemics, the LAC countries have approved the Plan of action for the prevention and control of HIV and sexually transmitted infections 2016-2021 (17), which is aligned with the Global health sector strategy for sexually transmitted infections 2016-2021, whose goal is to end STI epidemics as major public health concerns (18).
In recent years, great strides have been made in the STI response—for example, screening of pregnant women for syphilis and improved surveillance of congenital syphilis. There is a firm political commitment to achieve the dual elimination of mother-to- child transmission of HIV and syphilis (19), and to provide greater access to vaccination against the human papillomavirus. Almost 60% (16/27) of the LAC countries have national STI prevention and treatment strategies or plans, but fewer than half of them (11/27) indicate that they are consistent with the targets of the global strategy (to reduce the incidence of syphilis and gonorrhea by 90% by 2030, eliminate congenital syphilis, and guarantee over 90% HPV vaccination coverage).
Only 63% of the countries (17/27) report having strategies to actively search for the contacts of people with an STI, although all of them (100%) report offering HIV screening and distributing condoms in STI treatment centers (Figure 11).
Furthermore, 88% (25/27) of the countries indicate that they have STI treatment guidelines, although only a little more than half (59%, or 16 out of 27) are consistent with WHO recommendations. In fact, only a minority (four countries) have updated their guidelines in the past two years, and more than half have not done so for over five years. In the absence of up-to-date national guidelines, health care providers sometimes follow the international recommendations of WHO or the CDC.
Some 66% of the countries (20/30) use rapid syphilis tests to screen and diagnose pregnant women, and 42% (13/31) report using them with the key populations (Table 7 of the Annex).
Figure 11 / Response to sexually transmitted infections in Latin America and the Caribbean, 2016, by percentage and number of countries
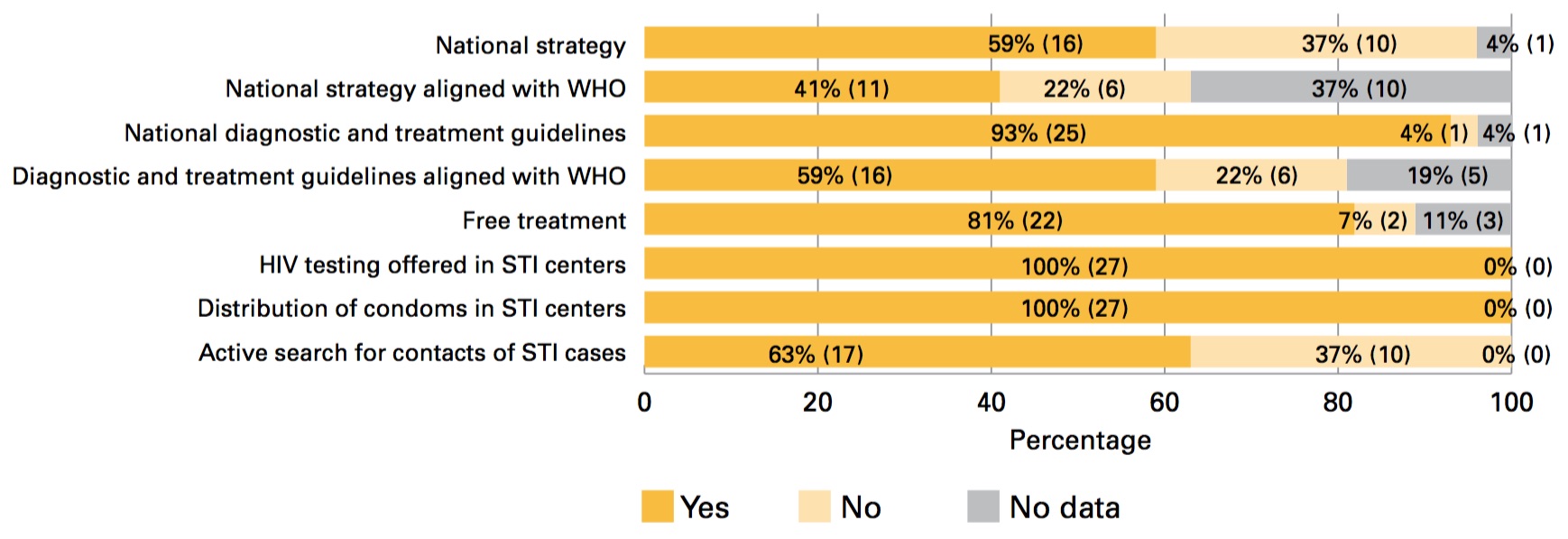
Source: PAHO. Country responses to HIV Prevention Survey, May 2017. Notes: National strategy = national STI strategy. National diagnostic and treatment guidelines= national guideline for the diagnosis and treatment of STIs. Free treatment = Treatment of STIs in the public health services is free of charge. The number of countries and territories in parentheses.
There are few data on STIs in LAC. Surveillance of these infections and response monitoring are inadequate, and even when surveillance systems are in place, they are sometimes characterized by deficient data and limited analysis and dissemination of the information.
Some 89% (32/36) of LAC countries report having some type of STI surveillance, and 88% (22/25) have designated active syphilis as a reportable event. Reporting syphilis in adults makes it possible to detect outbreaks and adopt effective targeted prevention and control measures. Congenital syphilis is reportable in the majority of the countries (94%, 30/32); only Haiti and Bolivia do not require reporting of congenital syphilis cases (Figure 12 and Table 8 of the Annex).

Figure 12 / Percentage and number of countries in Latin America and the Caribbean with surveillance of sexually transmitted infections, 2016, number of countries and territories
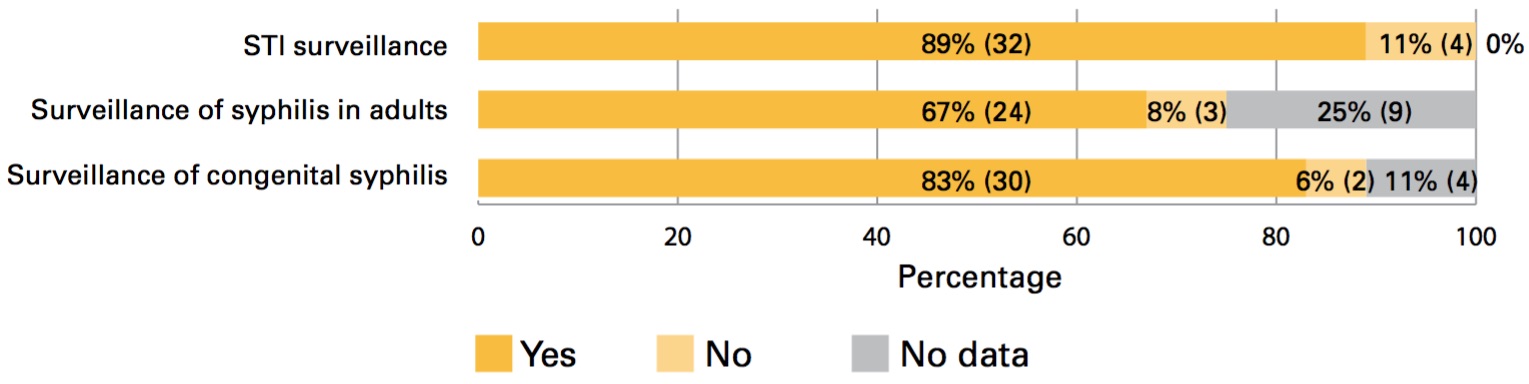
Source: PAHO. Country responses to the HIV Prevention Survey, May 2017; UNAIDS/WHO, Country reports, Global AIDS Response Progress Reporting 2016; PAHO, Elimination of mother-to-child transmission of HIV and syphilis in the Americas, Washington, D.C., PAHO; 2016. Note: The number of countries and territories in parentheses.
Table 7 / Surveillance of gonococcal resistance to antimicrobial drugs in Latin America and the Caribbean, by country, 2016

Source: PAHO. Data from the Latin American AMR Surveillance Network, 2009-2015. PAHO. Country responses to the HIV Prevention Survey, May 2017.
Of all the STIs, gonorrhea is the most antibiotic-resistant. This resistance has rapidly increased in recent years, reducing treatment options, and it varies with the different strains of Neisseria gonorrhoeae, making local surveillance essential to drafting guidelines for proper treatment. Cases of multi-drug- resistant N. gonorrhoeae have recently been detected that are unresponsive to monotherapy with broad-spectrum cephalosporins. WHO has published gonorrhea treatment recommendations suggesting that the choice of treatment in each country be determined by the local resistance data obtained through systematic resistance monitoring (21).
In LAC, 36% of the countries that provided information (12/33) conduct systematic surveillance of gonococcal resistance to antimicrobial drugs (Table 7). Furthermore, according to the country data reported through the Latin American AMR Surveillance Network (ReLAVRA), ciprofloxacin resistance has steadily grown, with isolates increasing from 35% in 2009 to 62% in 2015 (Figure 13). Moreover, reduced sensitivity to broad spectrum cephalosporins and macrolides is beginning to emerge (Figure 14).
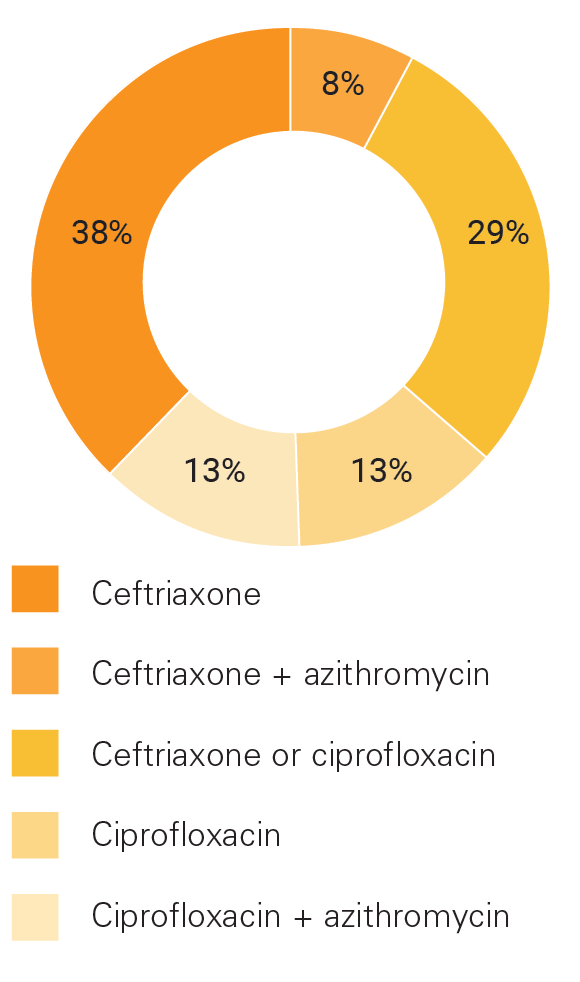
With regard to gonorrhea treatment guidelines, only 8% of the countries (2/24) report the use of ceftriaxone plus azithromycin, as recommended in the WHO guidelines; more than half (67%, 16/24) report the use of ceftriaxone or ciprofloxacin as the treatment of choice (Table 8 and Figure 15).
Figure 13 / Percentage of ciprofloxacin resistance in Neisseria gonorrhoeae isolates, Latin America and the Caribbean, 2009-2015
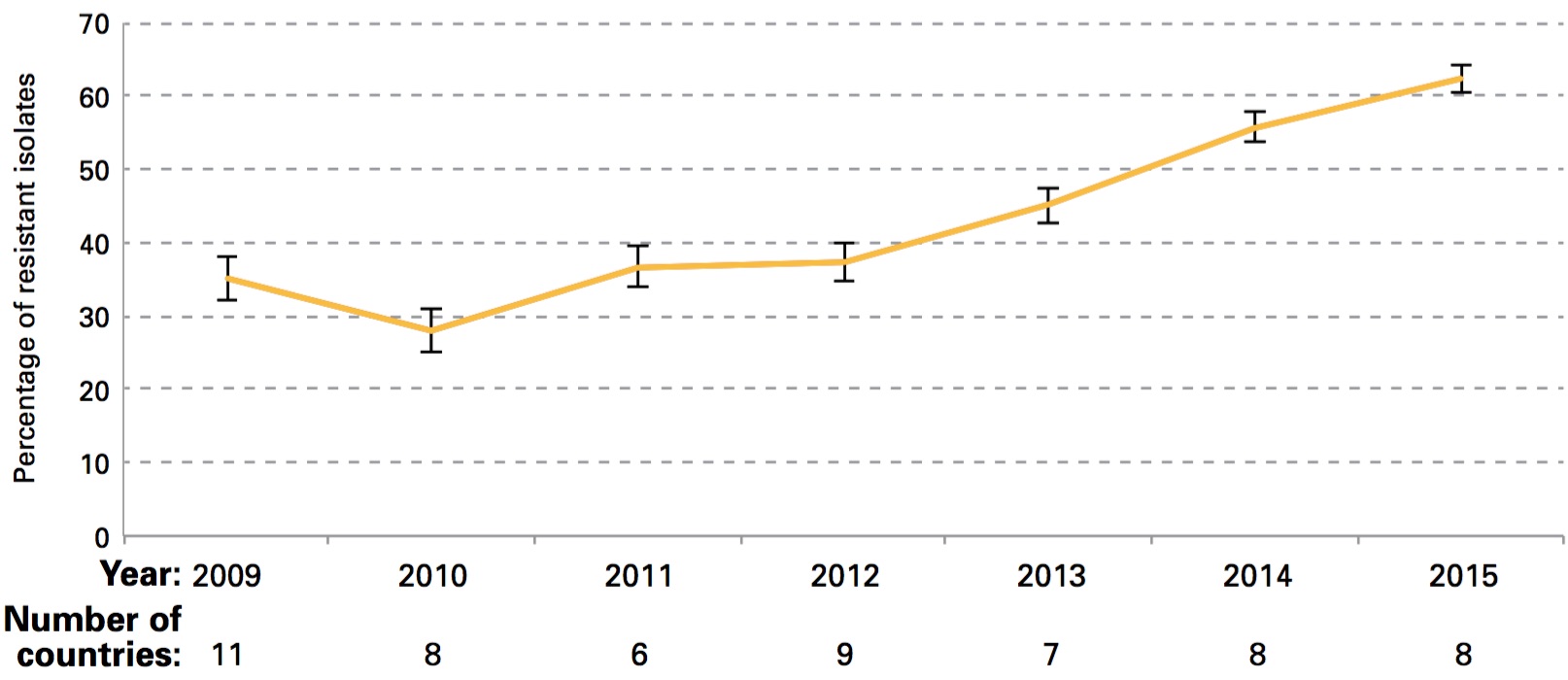
Source: PAHO. Data from the Latin American AMR Surveillance Network, 2009-2015.
Figure 14 / Percentage of azithromycin resistance in Neisseria gonorrhoeae isolates, Argentina and Chile, 2012-2016
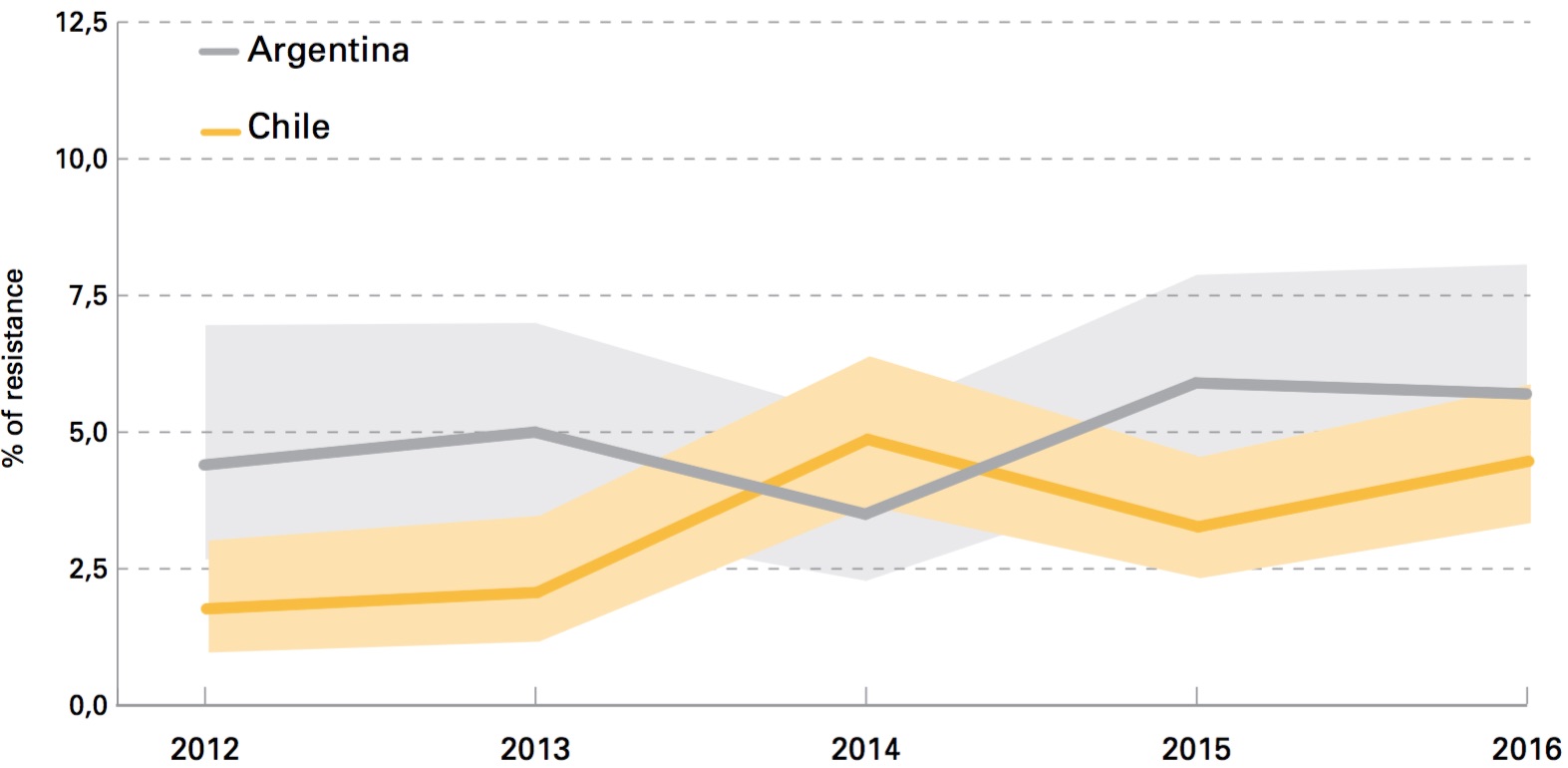
Source: PAHO. Data from the Latin American AMR Surveillance Network, 2009-2015.
Table 8 / Drugs for gonorrhea treatment indicated in treatment guidelines of Latin American and Caribbean countries
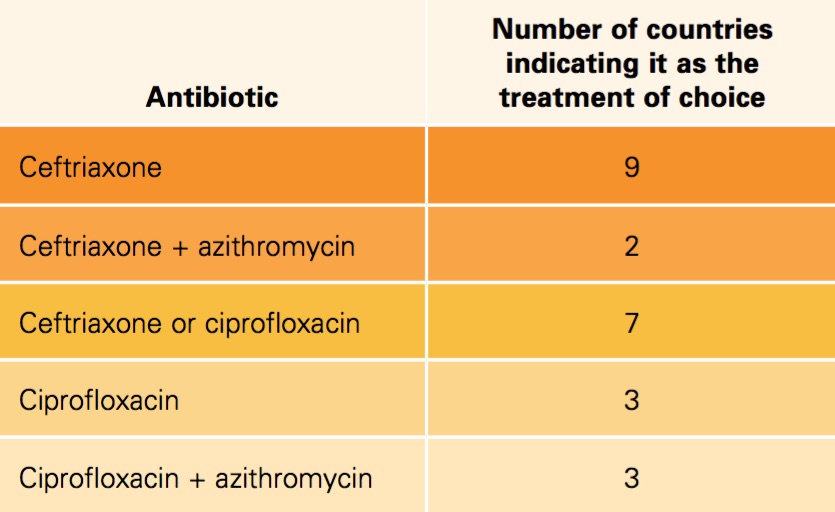
Source: PAHO. Country responses to the HIV Prevention Survey, May 2017.
Figure 15/ Percentage of countries by treatment plan indicated for gonorrhea, Latin America and the Caribbean, 2016
Pre-exposure prophylaxis or PrEP is the use recommends the use of antiretroviral drugs for HIV prevention in seronegative people. Who currently recommends the use of regimens that include oral tenofovir (e.g., tenofovir and emtricitabine), a drug widely used throughout the world for HIV treatment.
WHO (22, 23) recommends offering PrEP to people at high risk of contracting HIV as an additional intervention from the package of combination prevention interventions. This is a strong recommendation based on high-quality evidence.
In July 2017, WHO published a tool (24) for implementing PrEP programs with suggestions for the introduction and use of PrEP based on the available evidence and experience. This document includes information not only for clinicians, but for educators and activists, counselors, opinion- makers, pharmacists, regulatory agencies, planners and evaluators, HIV test providers, and PrEP users themselves.
PrEP is the use of antiretroviral drugs for HIV prevention in seronegative people.
Clinical trials and acceptability studies throughout the world show:
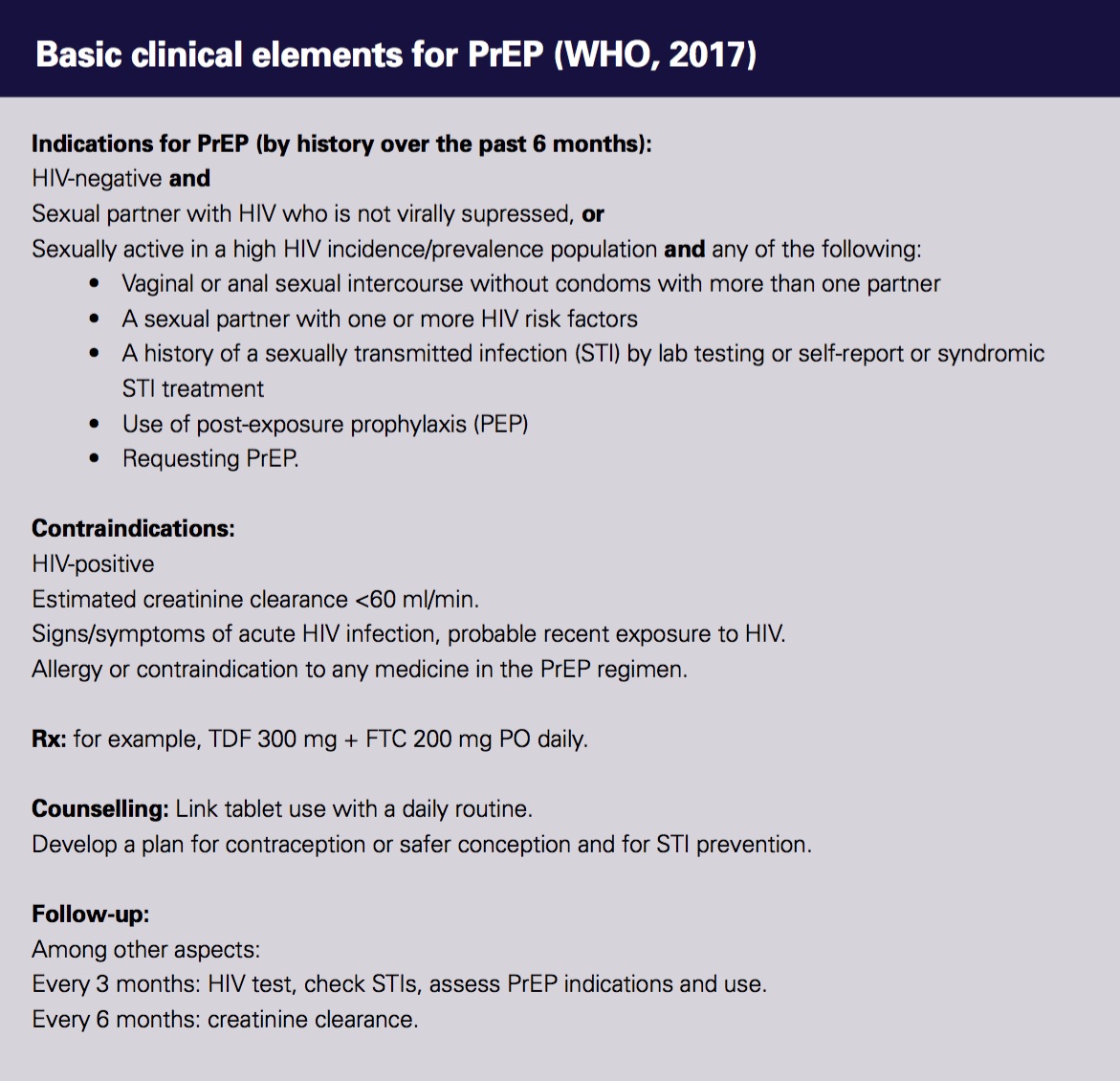
Source: WHO implementation tool for pre-exposure prophilaxis (PrEP) of HIV infection. Module 1: Clinical. 2017.
The use of PrEP as an intervention in HIV prevention packages is considered critical to the prevention response in LAC. Thus, having PrEP pilot projects in the countries is a first step, which is why it was set as a regional target in 2015 (see Table 1).
PrEP implementation has been slow (25) but is occurring in pilot demonstration projects for its adoption. It is also being offered in the public health services of the Bahamas and will soon be available in Brazil and Barbados (Table 9). The target of 10 projects is about to be reached. Seven countries are already planning public PrEP programs or projects with various modalities and sources of financing.

Source: PAHO. Key informants at 12 national meetings on prevention, 2017.
i) Quiero PrEP is available online at www.quieroprep.org/...
Table 9 / PrEP in public health services in Latin America and the Caribbean, 2017
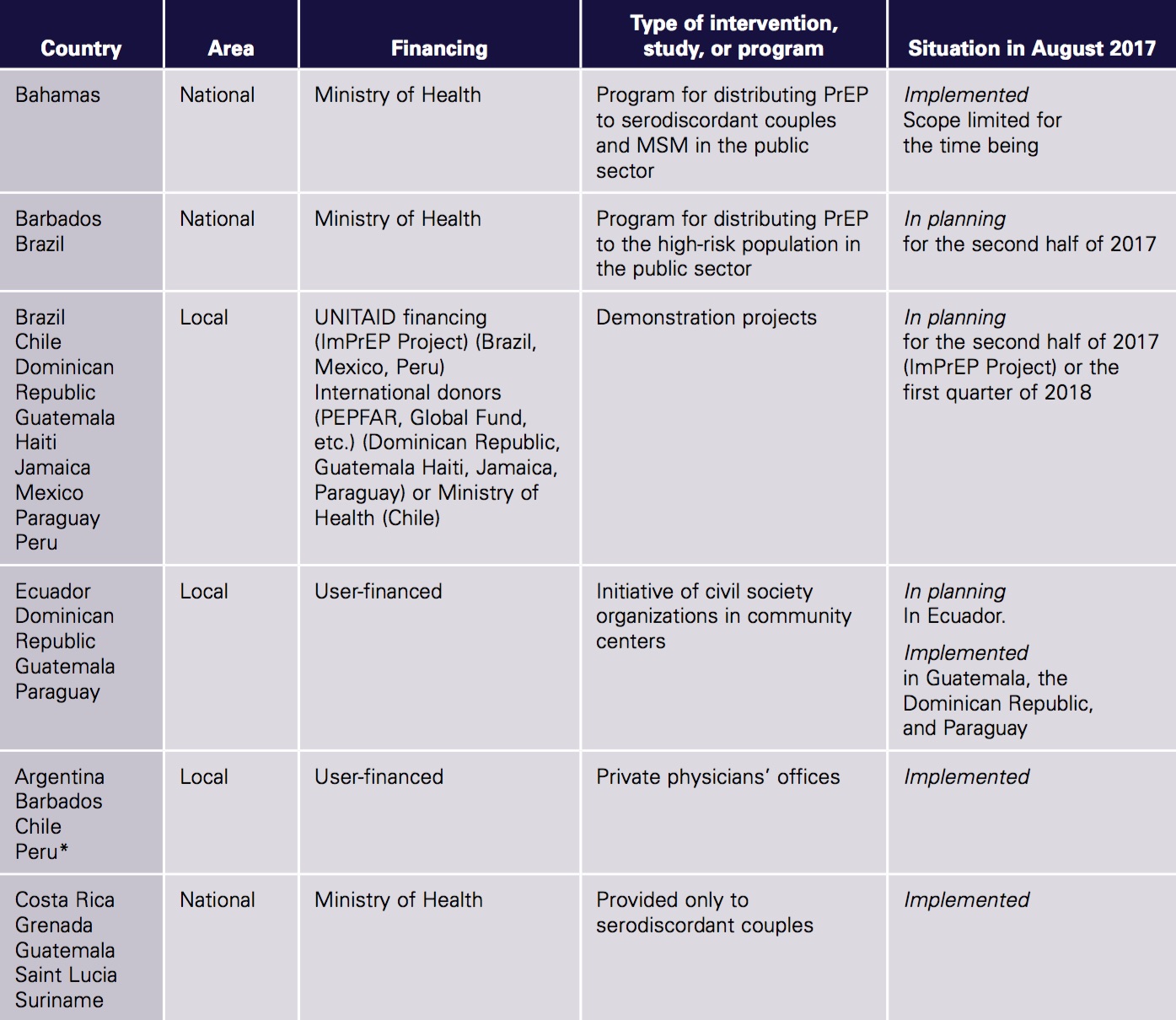
Source: PAHO. Direct information from the countries to PAHO. PrEP Network. Notes: * There may be more countries where PrEP can be obtained by prescription from private physicians. Dates in the table are approximate.
Several key informants have indicated that the number people who use PrEP outside the health sector has increased, a phenomenon known as “PrEP in the wild.” These users purchase the PrEP drugs in pharmacies and drugstores inside and outside the country or on the Internet, or else they obtain them through friends in social settings and self-administer them. This type of access does not guarantee compliance with the recommendations regarding interventions,
including, for example, providing information about their use, helping the patient continue treatment, monitoring side effects, and going for regular HIV and STI testing. Moreover, it does not enable national programs to monitor its use and outcomes. Other users obtain PrEP by prescription from a private physician, making it difficult to ensure the quality of care and adherence to national protocols and guidelines, which in many cases are still lacking.
Post-exposure prophylaxis (PEP) is the short- term use of antiretrovirals to reduce the probability of contracting HIV after potential exposure, either occupational (through a work related accident) or non-occupational (for example, during unprotected sex, rape, or the use of contaminated injection supplies). It should be administered within 72 hours of exposure.
All the countries provide PEP, either in primary care centers or emergency services for occupational exposure and rape. Some 39% (11/28) of the countries have adopted the WHO recommendation to provide PEP in cases of risk from unprotected sex (e.g., ruptured condom). Forty-two percent of the countries (11/26) stated their intention to increase the use of PEP, expanding the prescription criteria or the number of centers that offer it.
39% of LAC countries have adopted the WHO recommendation to provide PEP in cases of risk from unprotected sex
The most important measures for taking full advantage of PEP as a combination prevention strategy are as follows:
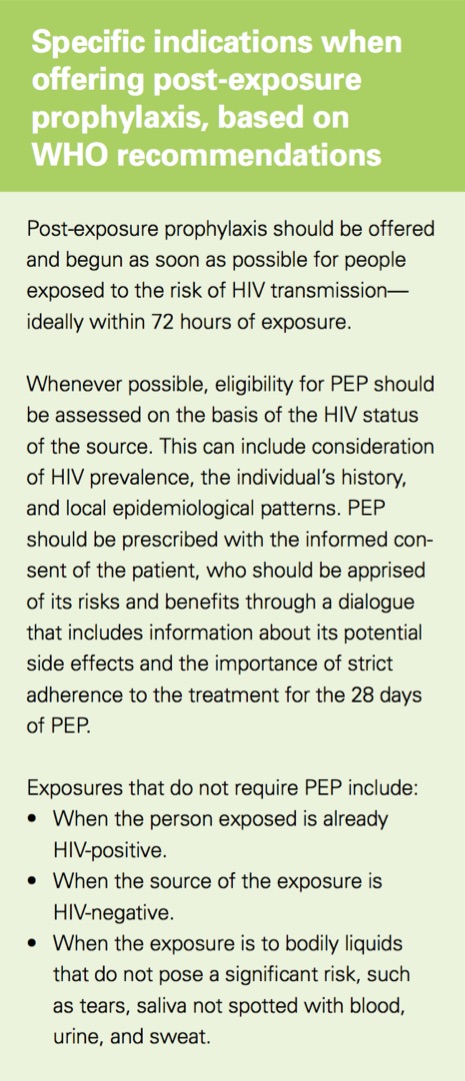
Source: WHO. Guidelines on post-exposure prophylaxis for HIV and the use of co-trimoxazole prophylaxis for HIV-related infections among adults, adolescents and children. Recommendations for a public health approach - December 2014.


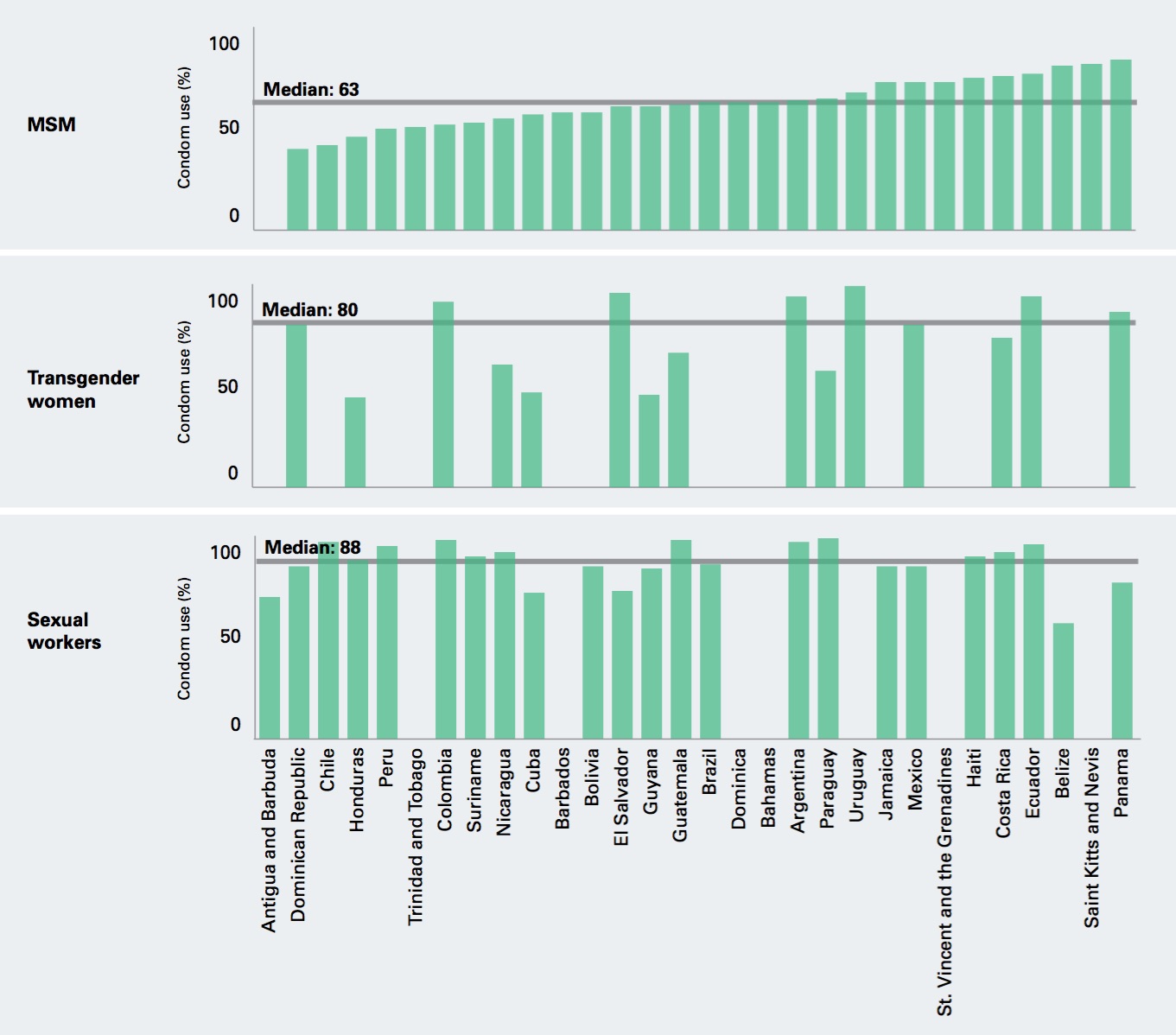
Condom use is critical for an effective integrated and sustainable approach to HIV prevention, and promoting it should remain a priority. The countries have made a commitment to promoting condom use to ensure that by 2020, 90% of FSWs report having used a condom with their most recent client. In the case of MSM and transgender women, the target is for 90% of them to have used one in their most recent anal sex with a male partner.
According to the latest available data in LAC, the regional median for condom use among MSM in their most recent sexual encounter is 63%; among FSWs, 80%; and among transgender women, 88%.
These data may include biases related to the representativeness of the study sample, differing definitions, the fact that the studies are often conducted in just a few urban areas (such as capital cities), a very lengthy interval between the years they were conducted, the methodology used in reporting the data, or other aspects related to the measurement indicator itself.
If data on the key populations seen in the services are used, the fact that these populations sometimes use these services to obtain condoms would make the result abnormally high due to selection bias. This indicator measures condom use in an individual’s most recent sexual encounter and is a proxy or indirect indicator of systematic use. However, it can overestimate systematic and timely use (Figure 16 and Table 9 of the Annex).
One-third of LAC countries reported procuring condoms with domestic resources.
Figure 16 / FSWs who report having used a condom with their most recent client, and MSM and transgender women who report having used one in their most recent anal sex with a male partner (%), most recent year available
In the key populations, it is essential to increase the availability, access, affordability, and use of the necessary number of male and female condoms and compatible lubricants through targeted distribution that supports proper and systematic use. Another priority is to promote access to condoms and lubricants by people who lack the resources to purchase them (7).

All LAC countries report providing free condoms (29/29) to MSM, and 28 out of 29 also provide them to FSWs. In the case of transgender women, 24 out of 28 countries report that they have distribution targeted specifically to this group. All the countries that provided information distribute free condoms to young people. However, according to the representatives of civil society organizations, in many countries the number of condoms distributed to MSM, FSWs, and transgender women is considered inadequate. The calculations for estimating the number of condoms and lubricants that should be procured are sometimes not tailored to the needs of the key populations or do not follow proven standard methodologies for this purpose.
The majority of the countries (25/28) report distributing lubricants. Colombia, Paraguay, and Venezuela do not distribute them to the key populations. In many countries, they are provided only by Global Fund projects, and eight countries (of the 26 that provided information) indicate that they do not distribute lubricants to young people.
One-third of the LAC countries (8/28) reported procuring the condoms with domestic resources. The rest provide condoms and lubricants with resources from the Global Fund or the U.S. government, primarily for those distributed to the key populations, as part of a prevention package.
Condoms are distributed mainly by the public health system as supplies for sexual and reproductive health programs. A smaller percentage (2%-35%) of condoms are distributed to the key populations by civil society organizations.
There are wide gaps in condom access and use, especially among the MSM population. This indicates the need to address the barriers to proper and systematic condom use and to offer complementary HIV prevention measures, such as PrEP.
The HIV epidemic, particularly in the key populations, is exacerbated by stigma and discrimination, gender-based inequality, violence, lack of community empowerment, human rights violations, and laws and policies that criminalize different groups of people based on their sexual orientation or gender identity (7). These factors hinder adequate access to health services, the way in which the services are provided, and the effectiveness of the services. Vulnerability to HIV is heightened if people are unaware of the available HIV prevention services or how to exercise their human rights.
The HIV response should consider the political, geographical, cultural, and social context that affects the risk of infection with the virus and access to services. The structural barriers (26) that hinder access to these services have been identified in the majority of the countries and can be summarized as:
A series of critical environment facilitators have been identified to address and overcome most of these structural barriers:
Effective implementation of critical facilitators requires collaboration among different sectors, including health, justice, housing, welfare, labor, and other sectors. It is also necessary for multiple stakeholders to work with the government, including civil society, the private sector, and people with HIV.
According to the GAM country reports, 10 countries (Bahamas, Bolivia, Colombia, Cuba, Dominican Republic, El Salvador, Mexico, Panama, Suriname, and Venezuela) report the existence of laws that criminalize transmission, nondisclosure, and HIV exposure. Seven more (Belize, Costa Rica, Grenada, Guatemala, Honduras, Jamaica, and Peru) do not have a specific law criminalizing HIV but have enacted other criminal legislation on HIV transmission, nondisclosure, and exposure.
Five countries (Antigua and Barbuda, Dominica, Grenada, Jamaica, and Saint Lucia)

RedTraSex is a network of local and national sex workers’ organizations that operates in 15 Latin American and Caribbean countries. In 2012, the network launched an HIV prevention program for FSWs through interventions for national defense workers. The program focused on three main activities:
RedTraSex has reached 17,306 FSWs through this methodology and held sensitivity training for 1,259 health workers in 14 countries. It has also produced a guide for health systems on good practices with FSWs. FSWs have participated to a greater extent in parliamentary debates. The principal changes brought about by these interventions are greater visibility of the problems facing FSWs (at the national and regional levels through their participation in the Organization of American States), improvements in the quality of care provided to them in health facilities, and the agreements signed with formal health systems.
Source: UNAIDS. Communities Deliver; 2015. Available from: www.unaids.org/...
Five countries (Antigua and Barbuda, Dominica, Grenada, Jamaica, and Saint Lucia) report that MSM run the risk of prosecution and prison. Civil society organizations in nine countries have reported cases of people who have been arrested or prosecuted in the past three years because they had sex with people of the same sex.
Six countries report that sex work is considered criminal behavior (Antigua and Barbuda, Bahamas, Barbados, Dominica, Grenada, and Jamaica) and four describe the partial criminalization of sex work (Bolivia, Costa Rica, Mexico, and Suriname). Civil society organizations in 15 countries report that female and male sex workers have been arrested or prosecuted for their sex work in the past three years.
Although no government reports the criminalization of transgender people, in the GAM reports, civil society organizations in nine countries (Antigua and Barbuda, Argentina, Costa Rica, the Dominican Republic, Honduras, Mexico, Paraguay, Peru, and Venezuela) state that in the past three years, transgender people have been arrested or prosecuted for activities related to their gender identity.
Of the 24 countries that provided information, 10 (Brazil, Colombia, Costa Rica, Dominica, Haiti, Honduras, Panama, Saint Lucia, Saint Vincent and the Grenadines, and Trinidad and Tobago) described access barriers to justice facing key populations and people with HIV. Some examples include barriers erected by the judicial system itself, which does not guarantee confidentiality; lack of trust in the judicial system; lack of sensitivity on the part of justice officials; and ignorance of judicial procedures.
One of the commitments assumed as part of the follow-up to the U.N. Political Declaration on HIV/AIDS in 2016 (29) was to empower people living with HIV, at risk of contracting it, or affected by it to know their rights and have access to justice and legal services in order to prevent and report human rights violations. In the past two years, 17 countries have reported having extensive training and capacity-building programs for people with HIV and the key populations to educate them and make them aware of their rights.
The goals established in the WHO Global Health Sector Strategy on HIV/AIDS 2016-2021:
m) Community empowerment is the individual and collective ownership of programs in order to achieve the most effective HIV responses and take concrete action to address social and cultural barriers to their broader health and human rights (WHO. Implementing comprehensive HIV/STI programmes with sex workers: practical approaches from collaborative interventions. Geneva; 2015. Available from: www.who.int/...
n) Definition of discrimination: Any action or omission by an individual or institution (for example, in the health sector) that produces and reproduces inequalities in access to resources and services (Diccionario de la lengua española. 23rd edition. Madrid, Spain).
Note: Factors indicated by participants in the national consultations on HIV prevention in May-June 2017.
In this regard, the Joint United Nations Statement on Ending Discrimination in Health Care Settings demonstrates the commitment of UN entities to working together to help Member States adopt coordinated multisectoral measures to eliminate discrimination in health care settings.
According to representatives of the key populations, health services are not welcoming and in some cases, abusive, which explains why the demand among these groups is very low.
This unfriendly attitude is one of the main barriers to timely access to HIV and STI diagnosis and treatment in the key populations. These informants also identify the main facilitators of discrimination in the health sector as the lack of sensitivity training for health professionals; ignorance among health professionals and users about rights and current laws and regulations.
Inconvenient hours of operation; the institutional behavior of health center professionals and authorities; bias among professionals; difficulty lodging complaints and grievances; and, in some cases, the failure to recognize civil society organizations as key partners in improving services.
A number of civil society organizations in 25 LAC countries reported having a mechanism for reporting discrimination and human rights violations in health care settings, such as reporting procedures, compensation mechanisms, and grievance procedures or systems to protect and respect patient privacy or confidentiality.
A full 97% of the countries reported having sensitivity training for health workers who offer HIV testing to people in the key populations. However, given the way it is carried out, many stakeholders and studies question the effectiveness of these interventions in eliminating stigma and discrimination in the health services against the key populations (30-32).
According to the RedTraSex study in LAC (33), 75% of FSWs obtain care through the public health system, where they have encountered the following types of discrimination:
According to the RedTraSex study in LAC (33), 75% of FSWs obtain care through the public health system, where they have encountered the following types of discrimination:
Based on the comments of consultation participants, these training activities are neither monitored nor evaluated, and high staff turnover means that many health workers do not receive any training. The participants considered the strategy of hiring peer counselors and community navigators to be successful, as these individuals improve knowledge and understanding of the needs of each population and provide ongoing sensitivity training and interventions that actively involve the key populations and people living with HIV in the design, implementation, and evaluation of health services. For example, the sensitivity training conducted by organizations of the key populations, such as RedTraSex, have been successful in reducing discrimination in the health services. In addition, the programs need policies and codes of conduct to discourage stigma and discrimination. Government and civil society representatives described protocols, resolutions, and standards for preventing and penalizing discrimination. However, many health professionals, center administrators, and users were unaware of their existence or how to apply them.
Violence against the key populations heightens the risk of HIV and STIo exposure (35). Multiple structural factors influence the vulnerability to violence, including discriminatory laws, institutional repression, cultural and social norms that legalize stigma and discrimination, as well as their coexistence with the activities of groups operating outside the law (for example, gangs in Central America). There are high rates of reported verbal and physical violence against FSWs and transgender women that sometimes result in death (36 ), as well as high rates of homophobic violence. For example, according to the Observatory of Murdered Trans People, 2,016 transgender people were murdered in the period 2008-2015, 1,573 (78%) of them in LAC (37). This reflects the gravity of the violence and crimes against trans people, which are correlated with the prevalence of HIV, late diagnosis of HIV, and the high level of mortality in this population.
Civil society organizations and national programs are working to reduce violence against the key populations and create an enabling environment that promotes physical, sexual, and emotional well-being, in addition to safety. There is an inherent constraint, however: health programs and services fall under the ministries of health, while uniformed personnel and programs to fight organized crime are under another portfolio. The directors and technical personnel of the programs consulted agree that lack of coordination among ministries and programs is a major constraint.
The critical facilitators for mitigating violence include: 1) mechanisms for documenting and monitoring violence; 2) training people in the key populations, people with HIV, and other stakeholders to understand human rights; and 3) strengthening intersectoral efforts to promote responsibility among law enforcement personnel to prevent violence and human rights violations.
As part of the efforts to prevent institutional violence in the health sector, it will be necessary to review policies and procedures for the application of standards, provide sensitivity training for professionals, train the key populations, and create human rights oversight mechanisms.
o) The Inter-American Commission on Human Rights (IACHR), the Inter-American Commission of Women (CIM), UNAIDS, and PAHO call on OAS Member States to eradicate stigma and discrimination surrounding HIV in the Americas (December 2012). Available from: onusidalac.org/...
The global targets in HIV prevention include allocating one-quarter of the HIV budget to prevention and ensuring that at least 30% of the services are community-operated by 2030.
Based on the data from 33 countries, UNAIDS estimates that LAC investment in the HIV response in 2013 was US$ 3 billion (38). Some 88% of the HIV expenditure was financed with domestic sources and 12% by international sources. In addition, 23% (US$ 690 million) of the expenditure allocated to the HIV response that year was devoted to prevention.p According to the data from the 23 countries that reported preventive expenditure targeted to the key populations, 7% of the expenditure on prevention in 2014 was allocated to programs for these populations (US$ 44 million of the US$ 639 million for prevention) (38).
With regard to the sustainability of the purpose, 68% of the countries (17/25)q have a dedicated budget line for this purpose in their HIV budget. However, 82% (27/33) depend on external funds for prevention, and only six countries finance 100% of their prevention activities with domestic funds (Table 10). This dependency is seen primarily in prevention for the key populations; the figure ranges from 5% in the Bahamas to more than 95% in Haiti, but in more than half the countries it is estimated at less than one-third of the total prevention funds.
Hence, we can see that we are faced with a dual challenge: first, reaffirming the political will to allocate domestic funds to financing in this area, and second, determining the real needs in order to increase the allocation for prevention in the key populations.
In 2014, funding for prevention activities in LAC was distributed among the key populations as follows: 6% for FSWs, 30% for MSM, 23% for the partners and clients of the key populations, 3% for transgender women, 2% for drug users, and 36% for the general population. The GARPR reports of several countries have indicated very little or no spending on prevention programs for the key populations. Some countries have difficulty quantifying the expenditure allocated to these populations and, based on the conclusions of studies in several of them (for example, GOALS and other similar studies), the proportion of the expenditure allocated to the key populations must be increased to ensure a greater reduction in new infections (39-43).
p) Considering only public funds, the percentage of the total allocated to HIV prevention is 20% and 28% in Latin America and the Caribbean, respectively.
q) According to information based on LAC country responses to the HIV Prevention Survey, May 2017.
Table 10 / Dependency of LAC countries on external funds for HIV prevention, July 2017
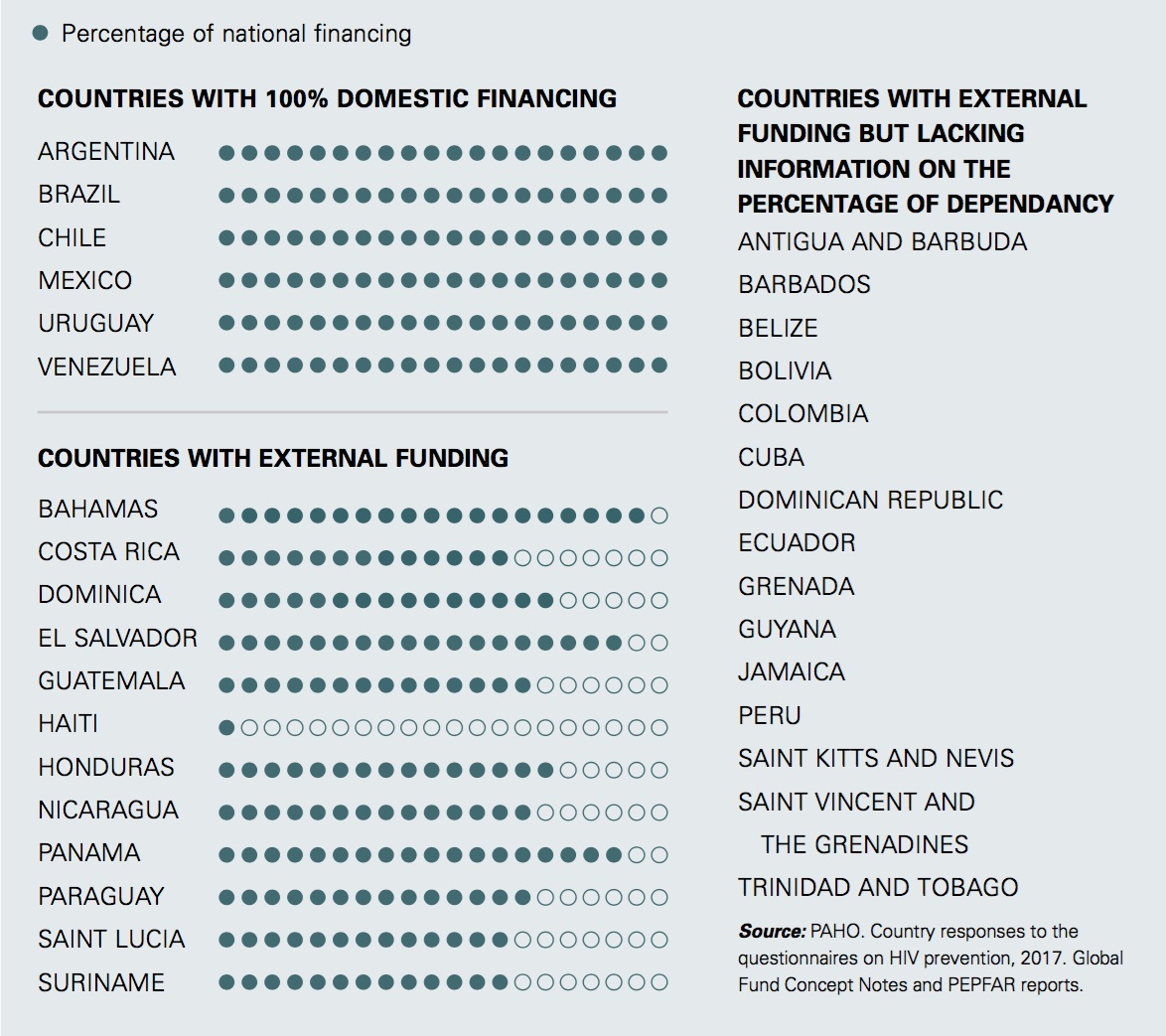

© Joshua E. Cogan
The countries also need to improve their information on the financing of HIV prevention—for example, by institutionalizing the development of national health accounts, using the methodology recommended by WHO (44) and considering systematic NASA exercisesr (at a cost of roughly US$ 5,000) or similar studies, whose low cost will enable them to monitor expenditures on prevention activities in key populations.
Furthermore, 60% of the countries (15/25) report that they have domestic resources to fund civil society interventions. In some countries, however, these funds take the form of supplies, and the amount of the financing has not been quantified.
r) NASA: National AIDS Spending Assessment. For more information, visit: www.unaids.org/...
In conclusion, in LAC, there is a high level of dependence on external funds for prevention activities targeted to the key populations, and inadequate funding for civil society
organizations, which are the most effective entities for reaching these populations. Some informants from the key populations in countries with 100% domestic financing stress the inadequacy of domestic financial support to civil society organizations for HIV prevention activities in these groups. Governments should create lines and mechanisms for funding civil society with domestic sources to support HIV prevention interventions, and countries that already have them should increase the funding, establishing fair and transparent mechanisms for the selection of service providers.
The current amount allocated to HIV prevention in key populations is insufficient; there are interventions that are not offered or if offered, the coverage is low.
This report analyzes the elements that show the main persisting gaps in HIV prevention in LAC. Use of the combination prevention approach can help LAC make progress toward meeting the 2020 and 2030 targets. However, given that two years after the LAC countries embraced the regional prevention targets, the number of new HIV infections has still not fallen, this report issues guidelines for reorganizing efforts and heightening their impact to achieve the sustainability of the outcomes. The following are the main areas where efforts should be focused in LAC:
There is a strong leadership by governments and civil society to end AIDS in LAC, but much remains to be done to improve the situation of the key populations and the quality of care in health centers. These are the pillars for mounting an integrated HIV and STI response in the coming years, which will require more and better information, as well as an increase in technical and financial resources. The conditions are ripe for implementing the combination prevention approach. We hope this report will serve as a catalyst for creating the mechanisms and structures recommended by the new Global HIV Prevention Coalition in its fast-track action plan to reach the targets for 2020 in this next phase of the response to the HIV epidemic.

Table 1 / HIV prevention targets for the subregion

Source: PAHO/UNAIDS. Regional prevention targets. Second Latin American and Caribbean Forum on the Continuum of HIV Care. Rio de Janeiro; 2015. * Appropriate and tailored to the local and cultural context.
Table 2 / Programming cascade by key group and country, Latin America and the Caribbean, most recent year available
The data on the size of each key population reported by the countries, the number of populations that the country considered reachable when preparing its concept note, and the goal for each population indicated in the concept note.
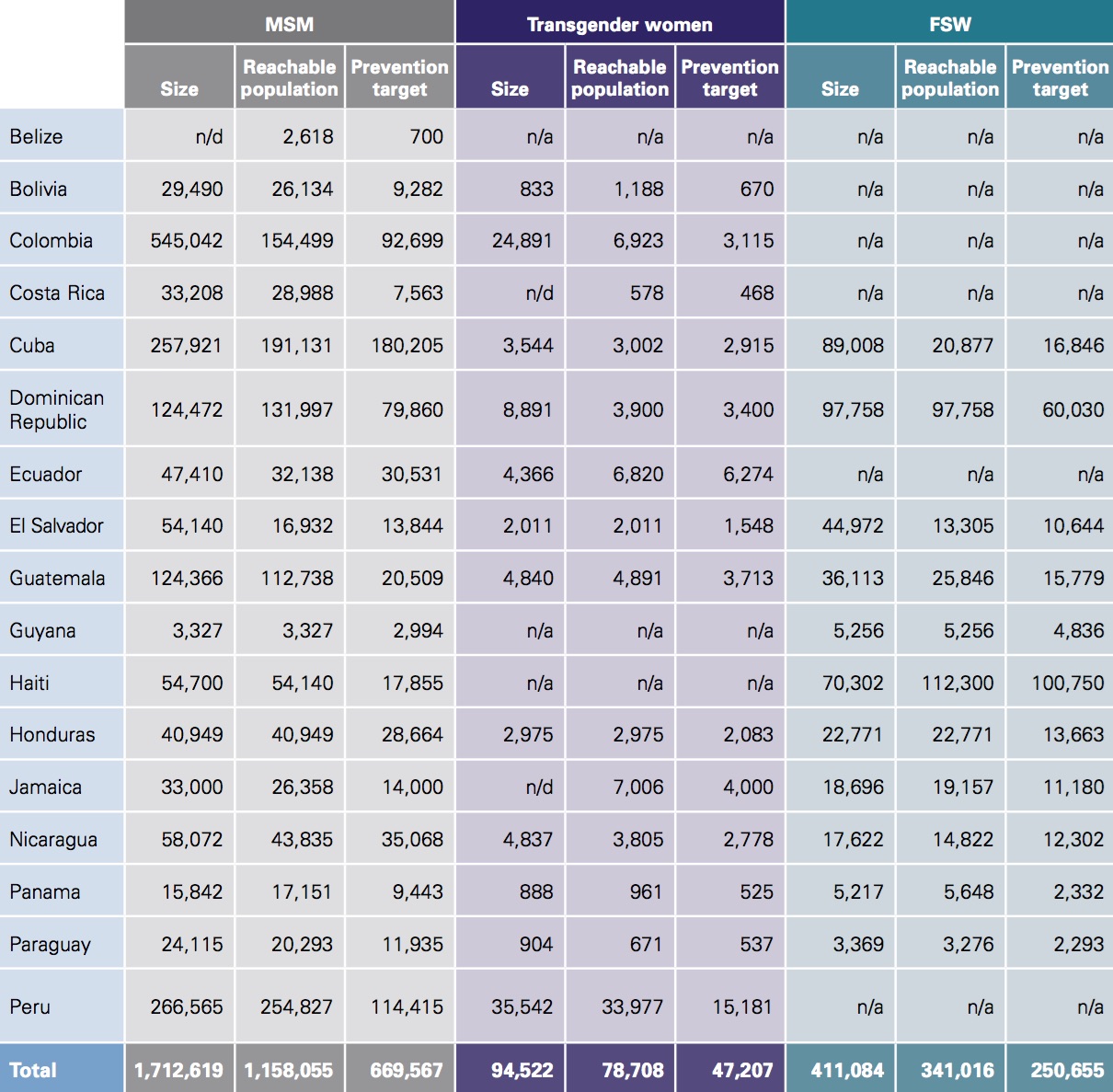
Source: Population size: GAM country reports; 2016. n/d: unavailable; n/a: not applicable or there is a grant from the Global Fund for these groups.
Table 3 / Percentage of men who have sex with men (MSM), female sex workers (FSW), and transgender women tested for HIV in the past 12 months in Latin America and Caribbean, most recent year available
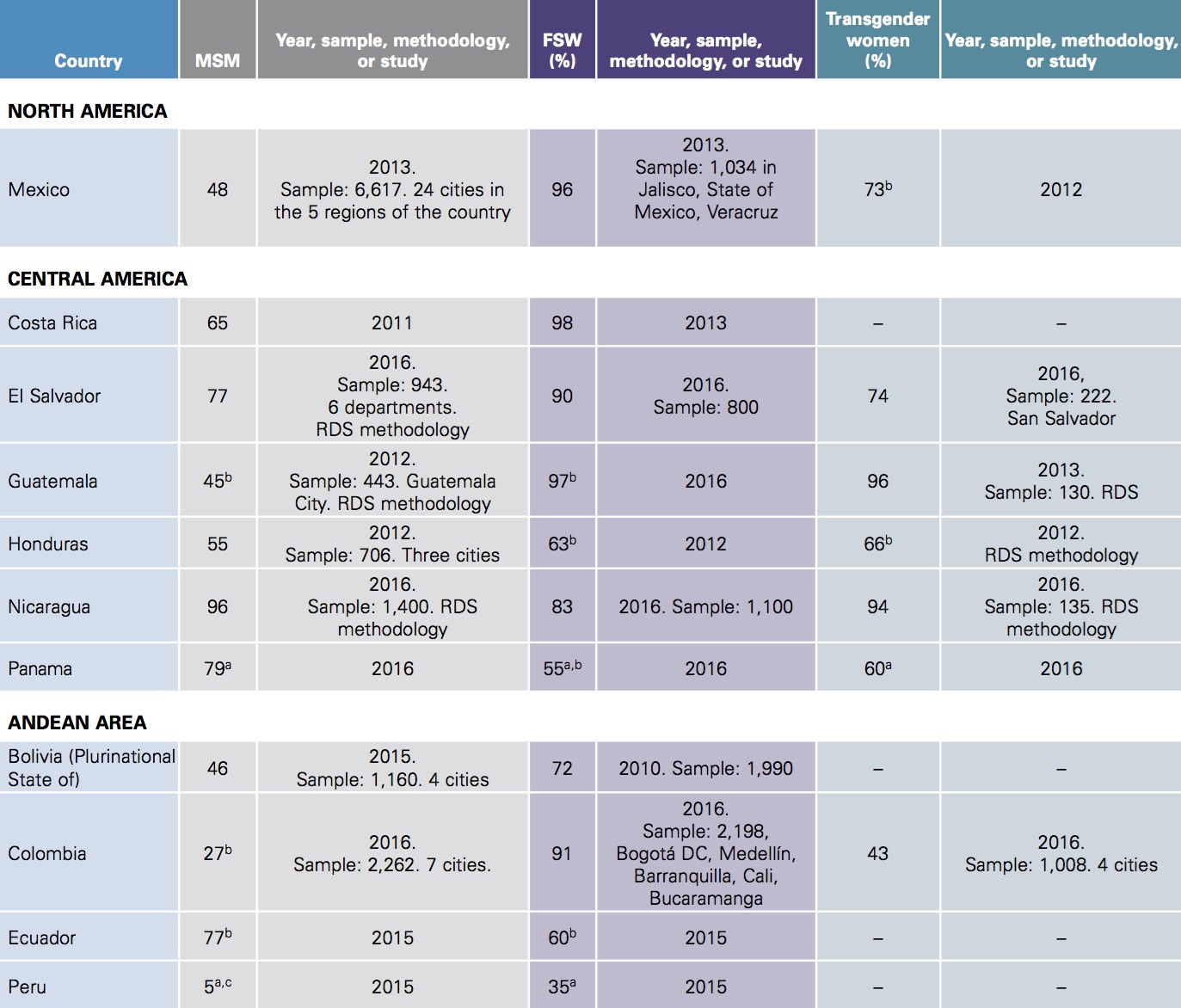
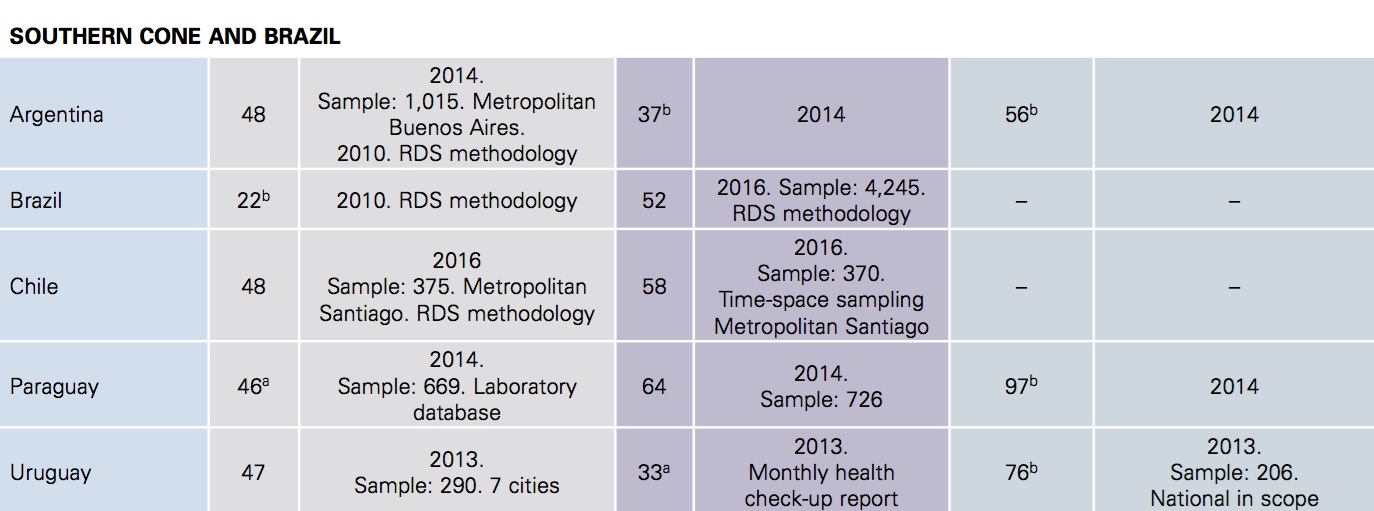
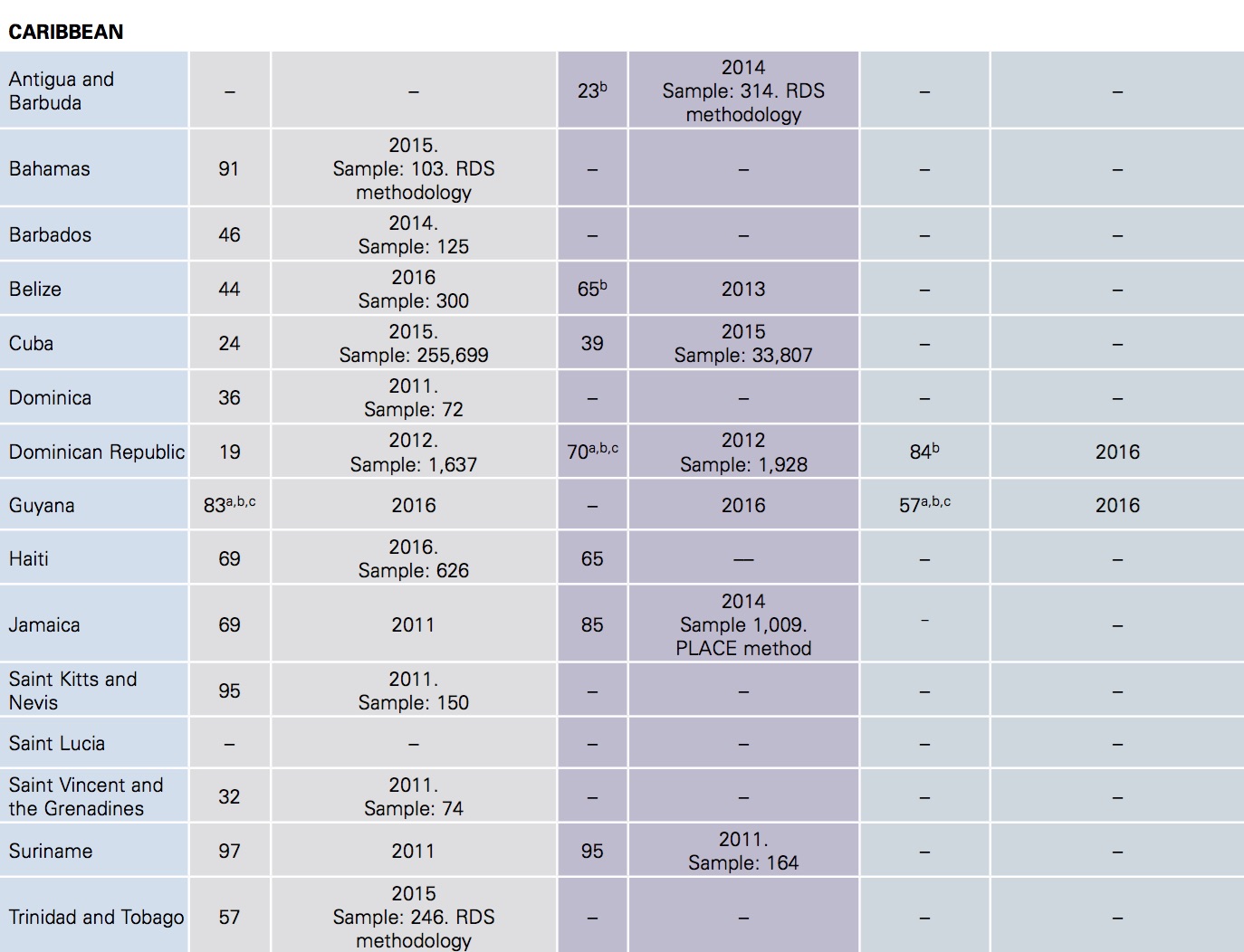
Sources: UNAIDS/WHO. Country reports, Global AIDS Response Progress Reporting 2011-2016; other sources of country data are indicated below. Notes: Data are based on surveys in selected cities, unless otherwise indicated. Different data collection methods (that is, RDS, PLACE, grab sampling), inclusion criteria, and sample sizes were used. a Data from programs for care to key populations. b Data reported directly to PAHO. c Numerator: Data from the testing and counseling service. Denominator: estimate of population size.
Table 4 / Active syphilis prevalence in gay men and other men who have sex with men in Latin America and the Caribbean, 2010-2016

Source: UNAIDS/WHO Country reports, Global AIDS Response Progress Reporting 2013-2016; other sources of country data are indicated below: n/d: no available data; VICITS: Sexually Transmitted Infection Surveillance, Prevention, and Control Strategy.
Table 5 / Active syphilis prevalence in female sex workers, Latin America and the Caribbean, 2010-2016

Source: UNAIDS/WHO. Country reports, Global AIDS Response Progress Reporting 2016. Note: n/d: no data.
Table 6 / Syphilis prevalence in pregnant women in Latin America and the Caribbean, 2015-2016
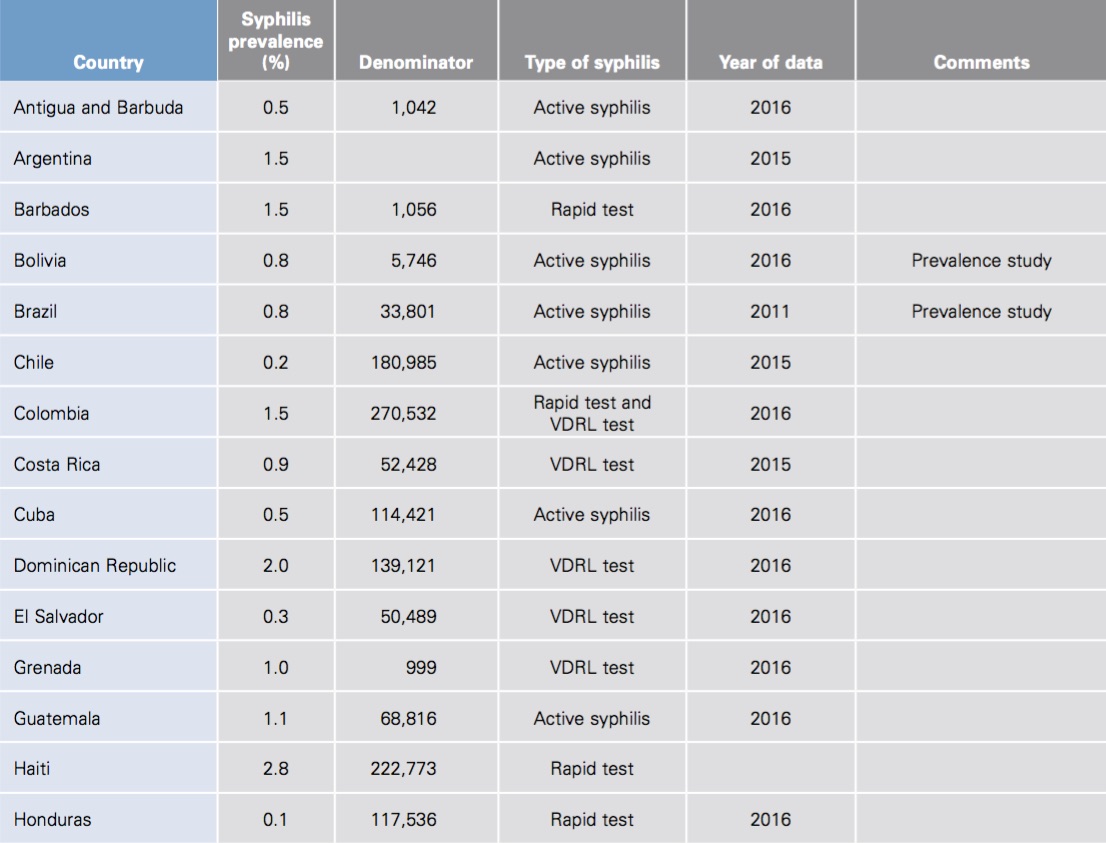

Source: UNAIDS/WHO. Country reports, Global AIDS Response Progress Reporting 2016.
Table 7 / Availability of rapid syphilis tests in Latin America and the Caribbean, 2016
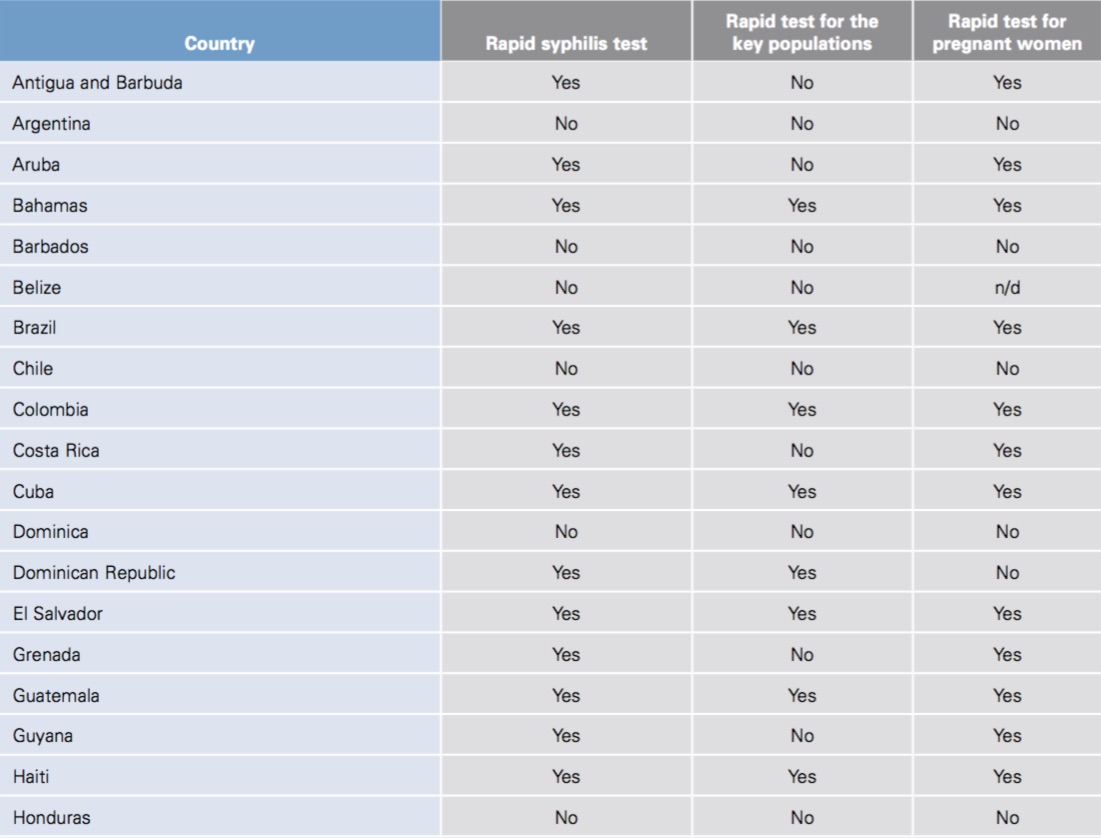
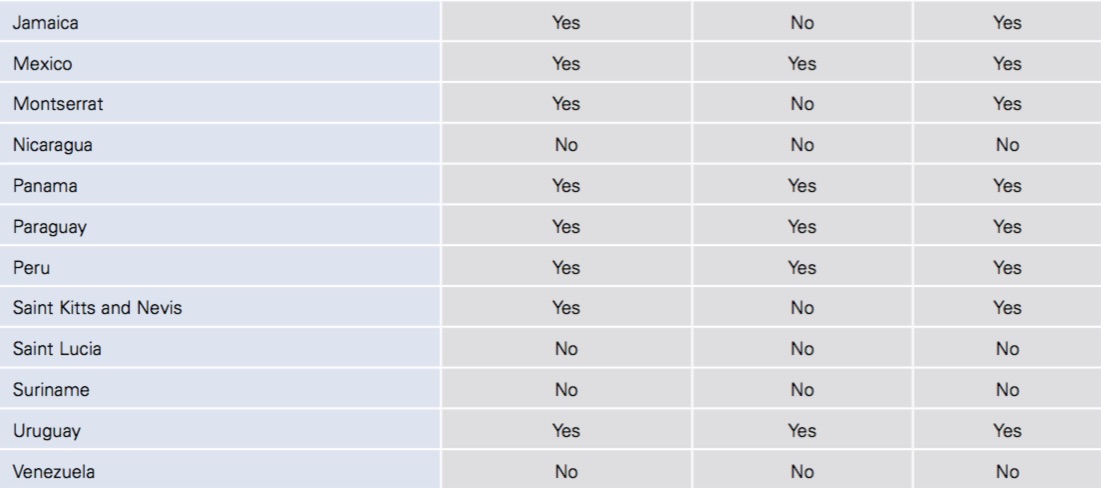
Source: PAHO. Country respnses to the HIV Prevention Survey, May 2017. PAHO. Elimination of mother-to-child transmission of HIV and syphilis in the Americas. Washington, D.C., PAHO; 2016. PAHO. Direct communication with countries. n/d: Unavailable.
Table 8 / Epidemiological surveillance of sexually transmitted infections (STI) in Latin America and the Caribbean, by country and territory, 2016
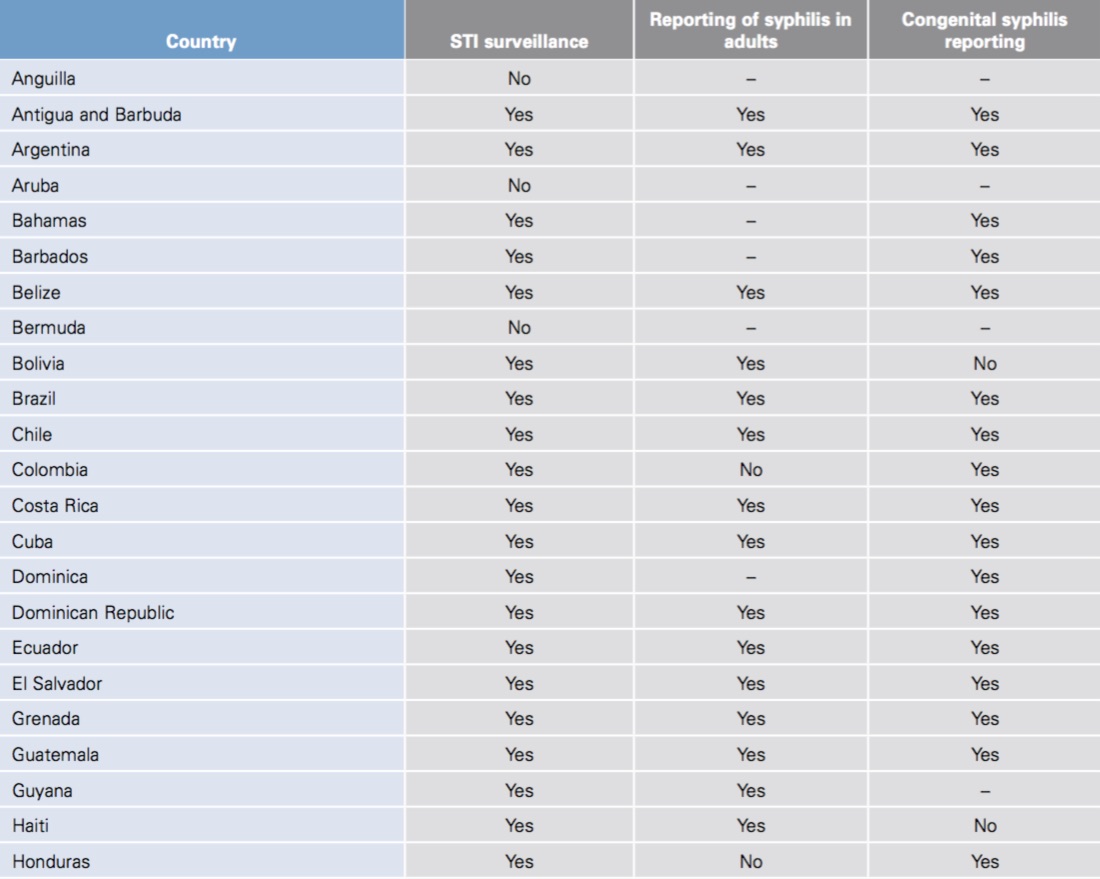
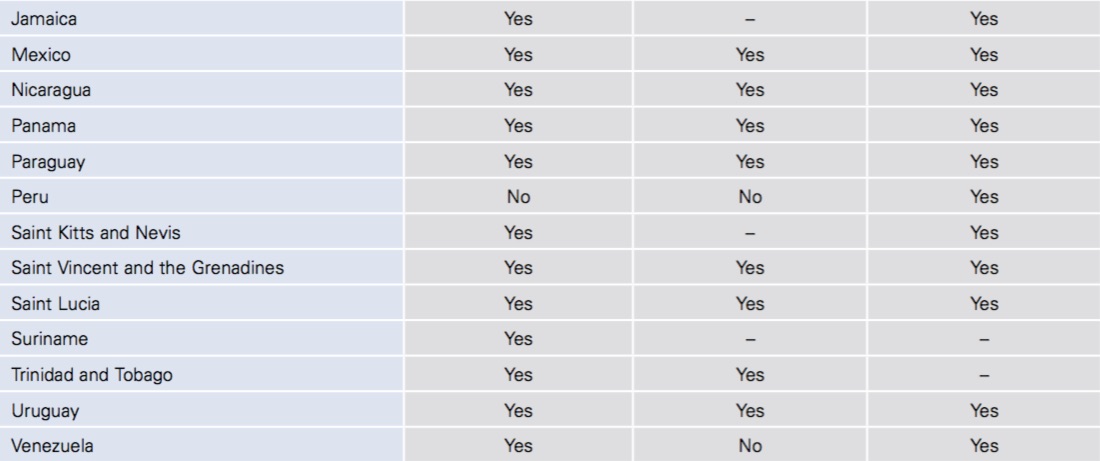
Source: PAHO. Country responses to the HIV Prevention Survey, May 2017. UNAIDS/WHO. Country reports, Global AIDS Response Progress Reporting 2013-2016. PAHO. Elimination of mother-to-child transmission of HIV and syphilis in the Americas. Washington, D.C., PAHO, 2016.
Table 9 / Percentage of female sex workers (FSW) who report having used a condom with their most recent client, and of men who have sex with men (MSM) and transgender women who report having used a condom in their most recent anal sex with a male partner, most recent year available

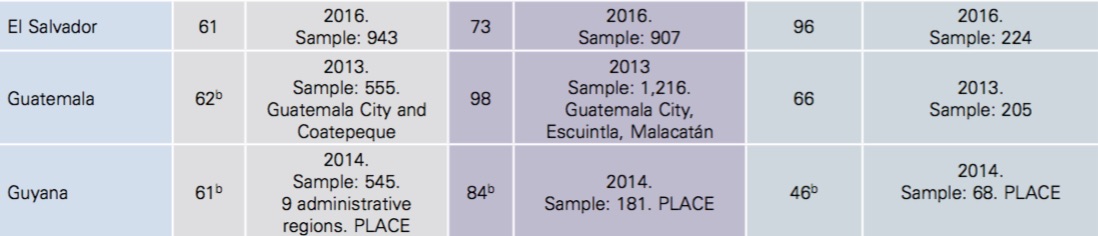

Sources: UNAIDS/WHO. Country reports, Global AIDS Response Progress Reporting 2011-2016; other country data sources are indicated in the table: a) Data from programs for care to the key populations. b) Data reported directly to PAHO. c) Condom use with a steady partner. Notes: Data are based on surveys in selected cities, unless otherwise indicated. Different data collection methods (that is, RDS, PLACE, grab sampling), inclusion criteria, and sample sizes were used. The percentages have been rounded.
All online documents were consulted on 11 October 2017.